An immunosuppressed person is one whose immune function is impaired by underlying disease and/or immunosuppressive medications, resulting in reduced immunosurveillance against malignant cells and increased vulnerability to opportunistic infections. Longstanding immunosuppression has been linked to increased risk for cutaneous (among other) malignancies for over half a century.1 Intrinsic patient characteristics, including advanced age, lighter skin phototype and personal and family history, shape baseline risk for many skin cancers.2,3 In addition to these factors, the main environmental risk factor for cutaneous malignancies, ultraviolet (UV) radiation exposure, causes immunosuppression in the skin, leading to a tumourigenic environment.4 Other conditions associated with skin cancers, such as xeroderma pigmentosum and Li–Fraumeni syndrome, can lead to markedly augmented risk over an individual’s lifespan.5
Epidermal malignancies are commonly categorized as melanoma, a neoplasm arising from melanocytes, and keratinocyte carcinomas, including cutaneous squamous cell carcinoma (CSCC) and basal cell carcinoma (BCC), that develop from keratinocytes.2,3 Less common cutaneous malignancies include Merkel cell carcinoma (MCC), a neuroendocrine neoplasm, and Kaposi sarcoma (KS), which derives from lymphatic endothelial cells. Immunosuppression has been implicated in other rare malignancies involving the skin, such as adnexal cancers, T-cell lymphomas and sarcomas, including angiosarcomas, leiomyosarcoma and pleomorphic dermal sarcoma.6–9 Though distinct, these cancers can occur in the same affected individual and share common characteristics, including immunologic underpinnings. For example, many cases of advanced melanoma, keratinocyte carcinomas and MCC respond favourably to immune checkpoint blockade (ICB) and are associated with high tumour mutational burden and inflamed tumour microenvironments.10
The mechanism by which immunosuppression promotes cutaneous malignancies is an area of active research. Available data suggest that impaired immune surveillance results in accumulation of UV-induced mutations and reduced tumour cell clearance.11 Viral oncogenesis may also play a role, such as the namesake Merkel cell polyomavirus and KS-associated herpesvirus in MCC and KS, respectively. Immunosuppressive medications can also drive mutation burden through direct DNA damage and, in some cases, increased UV photosensitization.4 Taken together, these factors can cause cutaneous field cancerization, such as where clonal proliferation of genetically altered keratinocytes develops into actinic keratoses, squamous cell carcinomas in situ and CSCC across a contiguous area of skin.12
In an ageing population, rising incidence of immunosuppression poses unique challenges for the diagnosis and management of cutaneous malignancies.13 Clinical presentation in immunosuppressed individuals may deviate from expected norms: skin cancers may appear at a younger age, in an atypical location, or with a more aggressive phenotype. Additionally, guideline-directed therapy for advanced cutaneous malignancies may be limited if ICB confers increased morbidity and mortality risk, such as in transplant recipients. Below, we broadly review risks for cutaneous malignancy by acquired immunosuppression subtype and implications for management (see key lessons summarized in Box 1).
Box 1: Key lessons
-
Immunosuppression is associated with substantially elevated risk of cutaneous squamous cell carcinoma (2–100×), Merkel cell carcinoma (4–24×), basal cell carcinoma (2–10×), melanoma (1–6×) and rarer malignancies, including cutaneous lymphomas and certain sarcomas
-
Skin cancer risk varies by aetiology, duration and intensity of immunosuppression, with differing risks in organ transplant recipients, those with haematologic malignancies, and those with autoimmune disease on immunosuppressive medications
-
Advanced age, lighter skin phenotype and cumulative ultraviolet exposure are established risk factors for melanoma and keratinocyte carcinomas that may synergize with immunosuppression to amplify risk
-
Real-world evidence from pharmacovigilance databases, registry studies and post-marketing surveillance is essential to characterizing skin cancer risk with novel immunomodulators, as clinical trials often exclude patients with prior malignancies and have limited follow-up duration
-
Multidisciplinary collaboration among primary care, dermatology, medical and radiation oncology, surgical subspecialties and transplant medicine can enable individualized risk stratification, screening interval determination, immunosuppression optimization and coordinated management of skin cancers in high-risk populations
Solid organ transplant recipients
Recipients of solid organ transplants experience an estimated twofold increased risk for overall cancer mortality compared with the general population.14 This burden will continue to grow as transplant survival improves and the at-risk population expands. Among cutaneous malignancies, solid organ transplant recipients (SOTRs) have a markedly elevated incidence of CSCC, KS and MCC, as well as modest increases in BCC and melanoma (Table 1).15–29 Skin cancers in SOTRs frequently present with more aggressive clinical and pathologic features, including multifocality, heightened risk of recurrence, nodal spread and increased disease-specific mortality.16,17 For example, SOTR status in MCC is associated with 24% mortality within 1 year of diagnosis, compared with 4% in non-SOTRs.18
Table 1: Risk for cutaneous malignancies by patient population

Relative risk ratios for skin cancer diagnosis compared with the general population are reported here based on the sources listed. Colour shading represents risk alteration: orange indicates increased risk, green indicates decreased risk, striped orange and grey indicates possible increased risk, and grey indicates unknown or insignificant change to risk. Darker colours correspond to greater magnitude of risk. Note that clinical trials assessing the safety of novel medications may exclude patients with prior cancer diagnoses, particularly melanoma; this may lead to bias in the available data described.
BCC = basal cell carcinoma; CSCC = cutaneous squamous cell carcinoma; IL = interleukin; JAK = Janus kinase; MCC = Merkel cell carcinoma; mTOR = mammalian target of rapamycin; TNF-α = tumor necrosis factor alpha.
As with other states of acquired immunosuppression, the increased incidence and aggressive phenotype of skin cancers may be driven by impaired tumour immunosurveillance resulting from chronic iatrogenic T-cell suppression. Certain immunosuppressants, such as calcineurin inhibitors, may exert direct pro-oncogenic effects (see below for medication-specific risk).30 As immunosuppression may unmask or accelerate occult malignancies, skin cancer screening of transplant candidates and recipients may optimize long-term outcomes per expert guidance.31
The Skin and Ultraviolet Neoplasia Transplant Risk Assessment Calculator (SUNTRAC) may be used to stratify SOTRs into risk categories based on race, age, sex, history of pretransplant skin cancer and thoracic transplant status; screening is recommended within 6 months of transplant for very high-risk patients (5-year skin cancer incidence of 45%) to within 10 years for low-risk patients (5-year skin cancer incidence of 1%).32,33 This calculator underscores the impact of age and lighter skin phototype in this at-risk population. For example, in a cohort study of >10,000 SOTRs, the 10-year cumulative risk of keratinocyte carcinoma development was <5% for patients aged 18–35 years, 27.5% for those aged 51–65 years and 40.5% for those >65 years of age at transplant.34 Skin phototype, which can be roughly approximated by race, also strongly impacts skin conditions affecting SOTRs, with malignant lesions predominantly presenting in white or Asian individuals.35
Management of advanced skin cancers in SOTRs requires a careful balance of graft preservation with oncologic control. Tailoring immunosuppression has been demonstrated to prevent and improve control of cancer-specific outcomes. While the optimal strategy remains unknown, dose reduction or transition to mammalian target of rapamycin (mTOR) inhibitor-based regimens are favoured approaches (see below for mTOR conversion).36 The mTOR inhibitor sirolimus is even the preferred first-line systemic therapy for advanced KS in SOTRs and may be sufficient for disease control with or without chemotherapy.37
Systemic therapy with ICB can be effective in some SOTRs but carries a substantial risk of allograft rejection.38 In real-world cohorts of kidney and liver transplant recipients treated with ICB, immune-related toxicity was found to be similar to non-SOTRs; an exception is acute graft rejection, which ranges in prevalence from 5% to 36%.39–41 Maintenance immunosuppression with steroids and mTOR inhibitors was associated with a lower risk of rejection compared with other immunosuppressant agents in one meta-analysis.41 ICB use in SOTRs requires multidisciplinary coordination, shared decision-making, consideration of graft type, baseline immunosuppression and alternative options, including standard-of-care therapies or clinical trials.
Persons living with HIV
Individuals who are HIV-positive are another population at elevated risk for cutaneous malignancies. Persons living with HIV (PLWH) are a well-established cohort affected by KS, which may involve the skin, mucosal surfaces and visceral organs. Beyond KS, PLWH experience significantly increased rates of MCC and CSCC. This risk elevation is heightened in the setting of poor disease control, characterized by low CD4 (cluster of differentiation 4)-positive T-cell count or high viral load. PLWH also tend to develop keratinocyte carcinomas at younger ages. They may present with more aggressive disease phenotypes than the general population, including in both CSCC and melanoma.23
Chronic HIV infection leads to persistent immune activation, depletion of CD4-positive T-cells and impaired tumour immunosurveillance, while concurrent viral infections also drive oncogenesis.42 Antiretroviral therapy (ART) may be central to modifying this risk.43 Specifically, ART-induced immunologic reconstitution may improve, but does not normalize, skin cancer risk.24,25 Residual immune dysfunction has been shown to persist even with strict virologic suppression.24,25
For advanced skin cancers, real-world evidence shows that ICB is both safe and effective in PLWH, with outcomes comparable to individuals who are HIV-negative when HIV infection is well-controlled.44 PLWH were historically excluded from clinical trials and remain a high-need population. Future ICB–based trials should broaden inclusion criteria to ensure equitable access to novel therapies in persons with well-controlled HIV infection.
Haematologic malignancies, including chronic lymphocytic leukaemia
Skin cancers are the most common type of secondary malignancy in individuals with haematologic malignancies. In a large retrospective analysis, nearly all haematologic malignancy subgroups showed more than a twofold increased risk of CSCC, BCC and melanoma compared with the general population.27 Elevated risks can persist for more than 30 years after diagnosis.27 Drivers of this association include disease- and treatment-related immune dysregulation, such as dysfunctional B cells, impaired antigen-presenting capacity and T-cell suppression. Shared oncogenic mutations, particularly those associated with poor prognosis in keratinocyte carcinomas such as TP53 (encoding the tumor suppressor protein p53), may also contribute.45
Among haematologic cancers, chronic lymphocytic leukaemia (CLL) confers the highest relative risk of diagnosis across all skin cancer types.27,46 In persons with CLL, CSCC, MCC and melanoma are often characterized by aggressive behaviour and worse outcomes than in the general population.28,47,48 The degree to which CLL-directed therapy can neutralize increased risk for cutaneous malignancies remains an active research area. Targeted agents (e.g. Bruton tyrosine kinase [BTK] inhibitors) appear to lower skin cancer risk when compared with chemo-immunotherapy (e.g. the fludarabine, cyclophosphamide and rituximab [FCR] regimen).45 On the contrary, ibrutinib with or without venetoclax has still been linked to increased risk of melanoma and keratinocyte carcinomas.45,49
Select myeloproliferative neoplasms (e.g. polycythaemia vera, essential thrombocythaemia and myelofibrosis) have also been associated with increased risk of keratinocyte carcinomas, melanoma and MCC, among other haematologic malignancies.27,50,51 In a Swedish population-based cohort study, hazard ratios for development of keratinocyte carcinomas and melanoma were 2.8 (2.4–3.3) and 1.9 (1.4–2.7), respectively.50 As these and other retrospective data suggest a decline in keratinocyte carcinoma diagnoses after initial myeloproliferative neoplasm diagnosis, a detection bias may contribute to this elevated risk.51 In contrast, medications used to treat myeloproliferative neoplasms have been implicated in more latent skin cancer development. Hydroxyurea, also known as hydroxycarbamide, is thought to cause keratinocyte carcinoma development via direct DNA damage after several years of treatment.52,53 Long-term exposure to Janus kinase (JAK) inhibitors (e.g. ruxolitinib) is also linked to elevated keratinocyte carcinoma and MCC rates, particularly when prescribed for myeloproliferative neoplasms.49,54
Like SOTRs, allogeneic haematopoietic stem cell transplant (HSCT) survivors represent another population at increased risk of skin cancers. They exhibit markedly increased rates of CSCC and BCC, often developing precancerous lesions with high burden of actinic damage and subsequent aggressive clinical behaviour.29 Conditioning chemotherapy, total body irradiation and chronic graft versus host disease (GVHD) can all induce long-lasting immune dysfunction that may contribute to this risk.55 Prolonged use of systemic immunosuppressants, such as calcineurin inhibitors, mycophenolate, corticosteroids and JAK inhibitors, can further impair tumour immunosurveillance.30,49
For all patients with haematologic malignancies, dermatologic surveillance can be an important aspect of comprehensive care, with optimal screening frequency tailored to individual patient history and health system resource availability. Annual skin cancer screening is recommended by the US National Comprehensive Cancer Network guidelines for high-risk persons with CLL or patients treated with JAK inhibition.56,57 For those considering allogeneic HSCT, skin cancer counselling should be routine for pre- and post-transplant.55 If allogeneic HSCT survivors require ICB for advanced skin cancers, caution is warranted. Though not absolutely contraindicated, ICB has been associated with risk of triggering or exacerbating GVHD and increased mortality post-allogeneic HSCT.58 Close coordination with the bone marrow transplant team is critical to ensure safe and individualized management.
Autoimmune diseases and immunosuppressive medications
Individuals with autoimmune and chronic inflammatory conditions have an elevated risk of cutaneous malignancies due to the combined effects of disease-related immune dysregulation and the immunosuppressive therapies required for disease control.59 Risk varies across disease subtypes and is further influenced by type, chronicity and combination of medications (Tables 1 and 2). While confounding by indication remains a challenge to the retrospective study of this phenomenon, available data suggest stronger correlation among some immunomodulators than others.60 As clinical trials assessing novel medications often exclude patients with prior malignancy diagnoses (e.g. melanoma), prospective data on secondary malignancies may be limited. Post-marketing pharmacovigilance studies are important for identifying real-world and longitudinal skin cancer risks in this context.54
Table 2: Risk for cutaneous malignancies by immunosuppressive medication
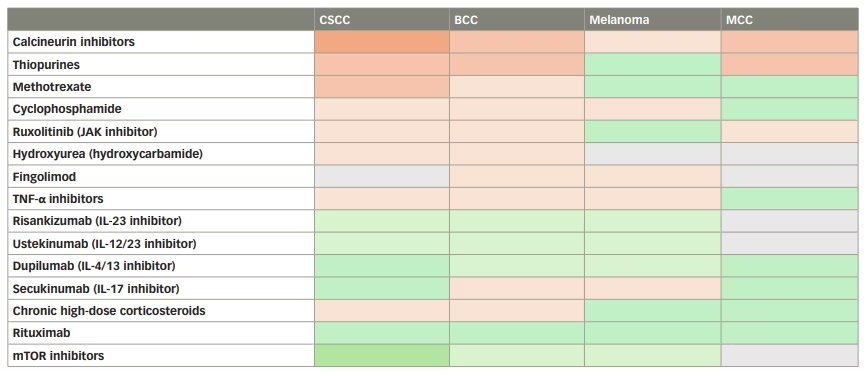
Relative risk ratios for skin cancer diagnosis compared with the general population are reported here based on the sources listed. Colour shading represents risk alteration: orange indicates increased risk, green indicates decreased risk, striped orange and grey indicates possible increased risk, and grey indicates unknown or insignificant change to risk. Darker colours correspond to greater magnitude of risk. Note that clinical trials assessing the safety of novel medications may exclude patients with prior cancer diagnoses, particularly melanoma; this may lead to bias in the available data described.
BCC = basal cell carcinoma; CSCC = cutaneous squamous cell carcinoma; IL = interleukin; JAK = Janus kinase; MCC = Merkel cell carcinoma; mTOR = mammalian target of rapamycin; TNF-α = tumor necrosis factor alpha.
Available data suggest that medication-specific mechanisms contribute substantially to skin cancer susceptibility.30,49 Thiopurines (e.g. azathioprine, 6-mercaptopurine) and calcineurin inhibitors (e.g. tacrolimus, cyclosporine) confer among the highest risk among immunosuppressive medications and across skin cancer subtype.30,54 Both methotrexate and the alkylating agent cyclophosphamide increase the risk of keratinocyte carcinomas (and for methotrexate, melanoma). Sphingosine-1-phosphate receptor modulators, such as fingolimod used to treat multiple sclerosis, are also associated with increased skin cancer risk, particularly BCC and melanoma in post-marketing surveillance.61–63 Conversely, mTOR inhibitors may harbour a protective effect against certain skin cancers. This has been demonstrated for the secondary prevention of keratinocyte carcinomas in SOTRs in a randomized trial (TUMORAPA 1: Efficacy of Rapamycin in Secondary Prevention of Skin Cancers in Kidney Transplant Recipients; ClinicalTrials.gov identifier: NCT00133887) and other studies.36,64–66
Among biologic medications, tumor necrosis factor alpha, or TNF-α, inhibitors (e.g. etanercept, adalimumab, infliximab) are considered lower risk medications, yet are still linked to higher rates of CSCC and melanoma.49 The CD20 (cluster of differentiation 20)-directed antibody rituximab has mixed evidence regarding association with skin cancers in national cohort studies.54,67,68 Alemtuzumab, a monoclonal antibody that targets CD52 (cluster of differentiation 52) on immune cells, has been identified as potentially elevating risk for melanoma, while data are limited for other cutaneous malignancies.63 Natalizumab, which binds the α4-subunit of α4β1 and α4β7 integrins, also has limited data regarding associated skin cancer risk.
Among interleukin (IL) inhibitors, IL-23 (e.g. risankizumab) and IL-12/23 (e.g. ustekinumab) inhibitors are associated with lower rates of melanoma and keratinocyte carcinomas compared with TNF-α inhibitors.54,69 IL-17 inhibitors (e.g. ixekizumab, secukinumab) also demonstrate low and stable rates of melanoma and BCC in treated patients.54,70,71 The IL-4/13 inhibitor dupilumab has demonstrated a signal for cutaneous T-cell lymphoma in pharmacovigilance data, though this may be due to unmasking of pre-existing disease rather than a direct oncogenic effect.72 Risks associated with novel IL inhibitors, such as those targeting pure IL-13 (e.g. lebrikizumab, tralokinumab) or IL-31 (e.g. nemolizumab), are incompletely described due to limited long-term follow-up data.49,73
In comparison with other immunosuppressive medications, chronic corticosteroid exposure has a modest independent effect but can amplify the impact of other immunosuppressive agents.30 The risk of keratinocyte carcinomas may, however, increase with high cumulative corticosteroid exposure.30 Significant exposure may be quantified by >10–15 treatment courses or continuous treatment exceeding 1 month.30 Notably, administration of high corticosteroid doses (≥10 mg prednisone equivalent daily) reduces efficacy of ICB therapy, and thus concurrent use is generally avoided, except in the treatment of severe immune-related adverse events.74
Given the potential for cumulative risk, proactive dermatologic management is recommended for patients on chronic immunosuppressive therapies.75 This includes annual skin cancer screening, with more frequent surveillance considered for those with a history of skin cancers on high-risk therapies, such as thiopurines or calcineurin inhibitors.31 The benefits of screening must be weighed against the possible harms (e.g. diagnosis of cancers unlikely to become clinically meaningful during a patient’s lifetime and health system resource utilization). Rigorous photoprotection remains a cornerstone of prevention and is particularly important for thiopurine users due to ultraviolet A-mediated photosensitization. Therapeutic adjustment should also be considered; for example, when clinically feasible, discontinuation of thiopurines or transition to alternative agents (e.g. mTOR inhibitors in SOTRs) may reduce subsequent or recurrent skin cancer risk.36,64–66 Finally, use of ICB in patients with autoimmune disease requires close monitoring and careful shared decision-making. Risks of ICB include the potential for disease flare, underscoring the need for coordinated care between medical oncology and subspecialists managing the underlying autoimmune condition.74
Prevention, early detection and multidisciplinary management
Multidisciplinary collaboration is critical for early detection and optimal management of cutaneous malignancies in medically complex patients with multiple risk factors for immunosuppression (Figure 1). Surveillance strategies should be individualized to intrinsic and acquired risk factors and may vary based on resource availability. Across settings, increasing patient awareness of this risk and possible presentation of abnormal skin lesions is also vital. Patients should also be counselled on photoprotection and self-examinations.
Figure 1: Multidisciplinary skin cancer management in individuals with acquired immunosuppression
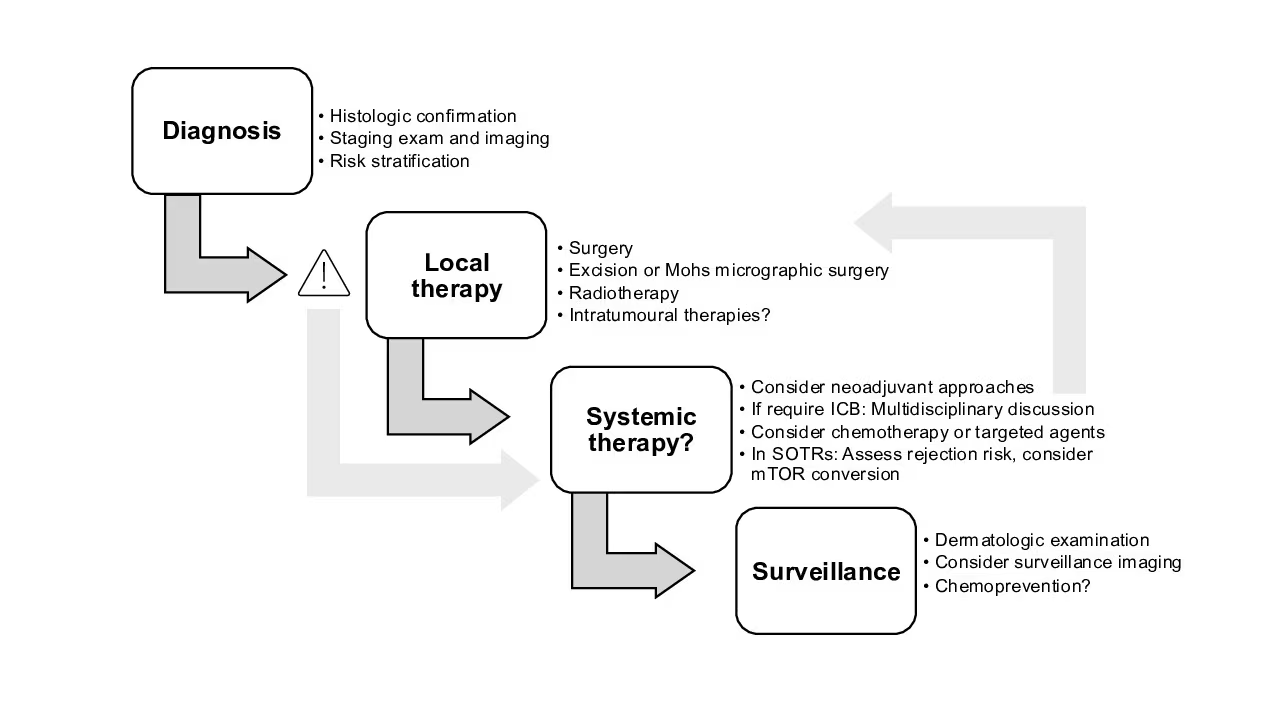
Figure 1 was created using Microsoft PowerPoint for Mac Version 16.107 (Microsoft, Redmond, WA, USA)
ICB = immune checkpoint blockade; mTOR = mammalian target of rapamycin; SOTR = solid organ transplant recipient.
Care for skin cancers begins before cancer develops. In addition to risk-minimizing behaviours and surveillance, precancerous lesions (e.g. actinic keratoses) may be addressed with topical treatments, cryotherapy or other local modalities.76 Field therapy, which addresses a larger area of actinic damage, may also be indicated with topical 5-fluorouracil, topical imiquimod or photodynamic therapy.15 In addition, the role of chemoprevention with nicotinamide or oral retinoids is also under evaluation for at-risk persons, such as those with a history of skin cancers.77 Although oral nicotinamide 500 mg twice daily did not reduce keratinocyte carcinomas in SOTRs in a phase III placebo-controlled trial (Effect of oral nicotinamide (vitamin B3) on skin cancer incidence and actinic keratoses in kidney, liver, heart and lung transplant recipients: a randomised controlled Phase 3 trial; ONTRANS: Oral Nicotinamide after TRANSplant; Australian New Zealand Clinical Trials Registry number: ACTRN12617000599370), the trial was stopped early due to poor recruitment.78 Chemoprevention with alternative doses, routes, agents or target populations merits further investigation.
Multidisciplinary management is also key in advanced cutaneous malignancies. Particularly in cancers affecting older persons, occurring on the head and neck region, or recurrent cancers in cosmetically sensitive areas, strategies that de-escalate or spare surgery without compromising outcomes are under investigation.75,79 Neoadjuvant or perioperative ICB for locally advanced CSCC and melanoma has been shown to elicit high pathologic response rates and improved event-free survival compared with upfront surgery.80–82 For individuals in whom ICB is contraindicated (e.g. certain SOTRs or severe autoimmune disease), aggressive local control is preferred and may include a combination of surgery, radiation and/or intratumoral approaches. Alternative systemic options may also be considered.75,79 These may include cytotoxic chemotherapy or targeted therapies (e.g. epidermal growth factor receptor [EGFR] inhibition with cetuximab, B-Raf proto-oncogene/mitogen-activated protein kinase [BRAF/MEK] inhibition in BRAF-mutated cancers or hedgehog inhibition in BCC). Treatment indication, response rates and tolerability vary by agent and tumour type.
Conclusion
Across subtypes of acquired immunosuppression, impaired tumour immunosurveillance, increased susceptibility to oncogenic viral infections and treatment-related effects converge to augment the burden of cutaneous malignancies. Older age and lighter skin phenotype remain well-established risk factors for many skin cancers, which can be additive to these risks. Unique causes of immunosuppression present distinct vulnerabilities: SOTRs face profound iatrogenic immunosuppression; PLWH contend with chronic viral immune activation; individuals with haematologic malignancies experience disease- and therapy-related immune dysfunction; and patients with autoimmune disease accumulate risk through long-term exposure to varied immunosuppressive regimens. These subgroups highlight the need for risk-adapted dermatologic screening and management guidelines that can be tailored to the underlying condition and treatment context.37,75,79 Equally essential are robust prevention strategies, early detection and timely local therapies. As novel biologic and targeted therapies continue to reshape the available treatment landscape, pharmacovigilance and longitudinal safety studies will be critical for refining risk estimates and optimizing skin cancer prevention and treatment for individuals with acquired immunosuppression.