




In haematologic malignancies with an unfavourable prognosis, high-dose chemotherapy followed by haematopoietic stem cell transplantation (HSCT) is the only realistic curative therapeutic option.1 Allogeneic and autologous haematopoietic stem cells are routinely used for transplantation. Allogeneic HSCT is associated with a significant therapy-related morbidity and mortality.2 In 2012, 6,482 stem cell transplantations were performed in Germany, and of these, 3,147 were primary allogeneic transplantations in children and adults.3
Until now, movement-related interventions as a supportive therapy were conducted either rarely, late or only on selected patients.4,5 During the acute inpatient phase of disease, such interventions have been applied in only a number of cases and in several institutions. Previous findings have confirmed the efficacy and safety of the use of movement-related interventions as a supportive therapy in the acute phase of carcinosis and as a form of motivation in maintaining a physically active lifestyle.5 The physical inactivity usually observed inevitably leads to a considerable reduction in physical capacity.6,7
Only a few studies have investigated the use of such interventions in patients undergoing HSCT.8,9 Prior to, during and following HSCT, patients experience an enormous amount of physical, mental and psychosocial stress, particularly a reduction in physical capacity, fatigue, emotional problems and haematopoietic and immunological changes.10,11 Prior to HSCT, the patient’s physical capacity is significantly lower than normal.12,13 In addition to other factors, physical capacity influences the health-related quality of life (HRQOL) and the overall performance of therapy.10,14
Previous studies that have addressed the use of movement-related interventions were primarily concerned with aerobic exercise.4,8 During the inpatient period, such interventions were able to stabilise the aerobic capacity of the patients, and a lower aplasia period and a reduction in fatigue were achieved.15,16,17 During high-dose chemotherapy, a significant reduction in the period of neutropaenia and thrombocytopaenia and the frequency of massive diarrhoea was observed following intervention with aerobic exercise.16
There have been only a limited number of studies that have addressed strength training during HSCT. Preservation of the physical capacity with interventions comprising of isometric strength training and a combined strength training and aerobic exercise have been performed.10,15,18
During the last decades, methods of whole-body vibration (WBV) training have generated much interest and are used practically in the fields of mass sport, particularly in line with therapeutic measures performed by physicians, physical therapists and sport.19,20 A rather high level of compliance is often observed with WBV training due to a number of advantages, which include its highly stimulative nature, and that it is less time consuming and subjectively less exhausting than conventional training. Furthermore, there is a minor degree of coordinative and specific capabilities that are required compared with other exercises.21 By engaging in WBV training, an increase in the muscular capacity (maximum force and speed and strength) can be similarly reached to that from strength training.21,22 The intensity of WBV training is regulated by the duration of each training session and the frequency, amplitude and body position in respect to the exercises performed on the device.19
From an organisational perspective, devices for WBV training are applicable in the inpatient setting because they require minimal space (2–4 m2) and are both easy to use and safe. Therefore, WBV training may be performed by patients autonomously following instruction.23
The aim of this study was to examine whether performing WBV training on every second day of hospitalisation, in combination with classic general physiotherapy, assists in stabilising the physical capacity of patients undergoing HSCT. The safety and suitability of such an intervention was also examined. Based on the findings of previous studies, we assumed that WBV training would have comparable positive effects on physical capacity, HRQOL and fatigue.11,24,25
Methods
The study was approved by the ethics committee of the University Medical Center Göttingen and was carried out following the guidelines for Good Clinical Practice (GCP) and the declaration of Helsinki. Participants were patients undergoing allogeneic HSCT at the Department of Stem Cell Transplantation, Clinic for Hematology and Oncology, University Medical Center Göttingen, Germany. Patients were eligible to participate in the study if they were to undergo allogeneic HSCT. Exclusion criteria were large unstable gallstones and nephroliths, thrombosis, fresh wounds, surgery within the previous 8 weeks, artificial joint replacements within the previous 6 months, stents and bypasses within the previous 8 weeks, coronary heart disease or arterial occlusive disease, insufficiently treated and uncontrolled hypertension, diabetes mellitus with complications such as advanced microangiopathy, gangrene, diabetic foot and retinal problems, osteoporosis of high degree with osteoporosis-related fractures, cardiac or brain pacemaker, pregnancy, under 18 years of age, clinically relevant blood coagulation disorders such as haemophilia, von Willebrand disease and thrombocytopenia with a platelet count less than 20 000/µl refractory to platelet transfusion, no signed consent form, osteolysis or fractures (e.g. from multiple myeloma), and an intrauterine device (<4 weeks after insertion of a device with one hook).
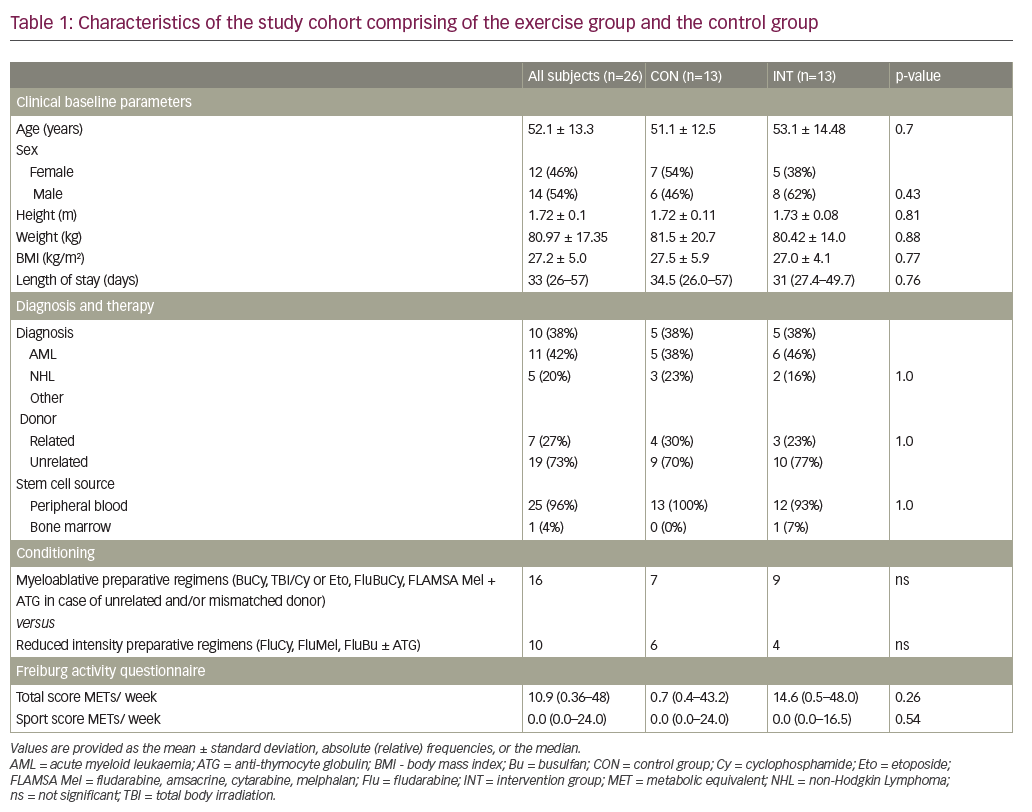
In this prospective, randomised, controlled study, 60 consecutive patients admitted to the stem cell transplantation unit between June 2008 and May 2010 were screened for eligibility. After verification of the exclusion criteria and a detailed medical clarification, 26 subjects provided written informed consent and were randomly allocated in a 1:1 ratio in an intervention group (INT; n=13) or a control group (CON; n= 3). The mean age of the patients was 52.1 ± 13.3 years, and the mean body mass index (kg/m2) was 27.2 ± 5.0. The descriptive data at baseline in the study cohort is described in Table 1. Data was collected upon admission and discharge. All instructions and recommendations given to the subjects were standardised.
Training program
Two Feel Well Board 3000 devices (Feel Well GmbH, Oberneufnach, Germany) were used for WBV training. Following completion of the study by one subject, the WBV training device was available for use for the next randomised subject. Included subjects were admitted to the respective ward for HSCT.
All patients were subjected to conventional physical therapy three to five times per week with each session lasting 20–30 minutes. Patients were requested to use a bicycle ergometer on a daily basis. The subjects in the INT group were also required to participate in WBV training every other day if possible and received a comprehensive instruction manual describing adequate use of the device, and a specific training schedule and training log for documentation of both WBV training and physiotherapy treatment. WBV training was performed under the guidance of a physiotherapist until subjects were able to safely and effectively carry out WBV training on their own. The intervention started on the first day of each subjects’ stay.
The training schedule comprised of a scheme for the progressive increase of the intensity and a constant variation in the training parameters frequency (10, 15, 20, and 25 Hz), amplitude 2–6 mm and duration (60, 90, and 120 s) to avoid a quick habituation of the body potentially reducing the effectivity of WBV training.21,22 The main progressive parameter was the frequency which increased from 10 to 25 Hz during the intervention. The training schedule can be found as supplementary digital content online (Supplementary Table 1). During each training session, four series were executed. No data on perceived exertion during the training sessions was collected. The intensity was increased by each subject themselves and individually according to the training schedule and given information. Subjects in the intervention group were instructed to use a basic position on the device (feet parallel on the device according to the feet position for choosing the amplitude, legs slightly bent, slightly lordotic posture, contraction of abdominal muscles, hands on the hand rails, head held erect) and to hold the position throughout each training set. Subjects were requested not to perform other dynamic or static exercises on the device to ensure that any observed effects are only attributable to the applied vibrations. To ensure that the individual absorption of various kinds of footwear do not adulterate the applied vibrations, subjects were advised to use the device wearing socks. The training schedule was designed in consideration of specific basics of the therapeutic-medical training theory to achieve an adequate quality assurance regarding implementation of the intervention.26 The intervention lasted for the whole hospital stay. Information regarding the length of the hospital stay can be found in Table 1.
The Board 3000 applies sinusoidal side alternating vibrations with a tilting platform on a mid-axis. It offers an eligible amplitude of 0– ± 6 mm depending on the foot position and a frequency of 5–25 Hz. The vibration parameters of the devices used for WBV training in this study were verified using a tri-axial accelerometer.27 Accelerations were mainly in the vertical direction and described an almost perfect sine wave. Significant divergences were found between the preset frequency and the actual applied frequency of between -20% and -27% in both devices. According to the manufacturer, these divergences were caused by a software failure that is no longer present in the follow-up models.
Biodex System 3
The Biodex System 3 (Biodex Medical Systems, New York, US) was used to measure the isokinetic performance in the dominant leg. Measurements were performed in accordance to the manufacturer and as previously described.28,29 Briefly, subjects were required to perform a 5-minute warm-up on a bicycle ergometer. All instructions and encouragement given to the subjects were standardised.
The concentric isokinetic flexion and extension of the knee of the dominant leg was tested at 60°/s, 180°/s, 240°/s and 300°/s.28,29 At each velocity, 5–10 submaximal flexions and extensions were performed for a proper warm-up and familiarisation, followed by two to three maximal warm-up and familiarisation repetitions.28,29 Subsequently, each subject executed five maximal repetitions for data collection with a break of 180 s between each heat.28 A range of motion between 0° extension and 100° flexion was aspired. Following an additional break, a muscular endurance tested was performed by recording the maximal number of repetitions reached across 60 s at an angular velocity of 240°/s.
The maximum peak torque (Nm), maximum relative peak torque (Nm/kg), and muscular endurance (number of repetitions, power [W]) were chosen. All subjects were required to undergo the identical test procedure.
Six-minute walk test
The six-minute walk test (6MWT) measures the maximal distance an individual is able to walk in 6 minutes. It is a submaximal test for the determination of the aerobic endurance performance capacity.30,31
Three repetitions were aspired and the subject was able to stop the test at any time.30,31 If a test was cancelled, the actual covered distance was recorded. If two or three repetitions were executed, the most optimal result was used for further analysis.
Health-related quality of life
The HRQOL was measured using the European Organisation for the Research and Treatment of Cancer Quality-of-Life Questionnaire-Core 30 (EORTC QLQ-C30) and comprises of 30 questions that have been specifically designed for patients with cancer.32 The EORTC QLQ-C30 covers five functional areas (physical, role, emotional, social, cognitive), three symptom scales (fatigue, pain, nausea and vomiting) and a global health and quality of life scale.32,33 Several single-item symptom measures are also included.
Freiburg activity questionnaire
The Freiburg activity questionnaire is a reliable and valid tool for determining the health effective physical activity of adults.34 Results of this test were the total score and the sport score both specified in metabolic equivalent (MET) per week. This questionnaire was only used upon admission.
Satisfaction and recording of unwanted side effects
Possible unwanted side effects of WBV training were recorded in a training log and regular contact with physicians and the physiotherapist. Furthermore, training sessions, the intensity of training and progress were documented. Causes of interruptions and compliance were also recorded. Satisfaction concerning the intervention was recorded via a questionnaire.35
Statistics
Statistical analyses were conducted using Statistica, Version 9.1 (StatSoft (Europe) GmbH, Hamburg, Germany) and SAS Version 9.2 (SAS Institute Inc. Cary, NC, US). All data of the CON and INT groups were compared according to the pre-specified analysis plan regarding the course of the study and with each other. The data of the Biodex measurements and 6MWT were analysed with a two-factor analysis of variance (ANOVA). The pooled changes from baseline to end of study in mean maximum relative peak torques in extension at all measured angular velocities were compared between the INT and the CON with a two-tailed t-test. A two-factor ANOVA was considered unnecessary in this case. The level of significance for all statistical tests was defined as a p-value of <0.05. Metric values from the subjects and analysis of the training log data were compared using a two-tailed Students t-test.
Results
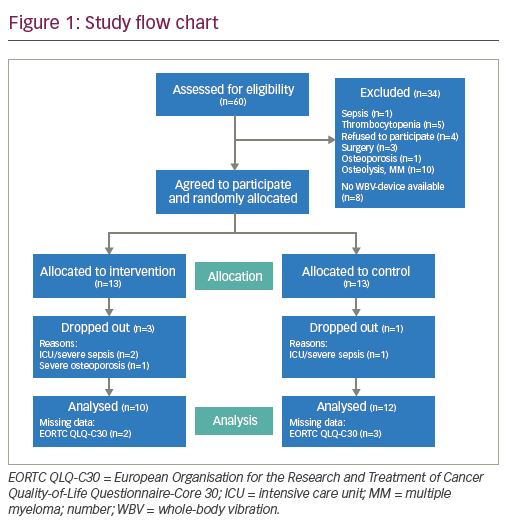
All following values are provided as the mean ± standard deviation (SD) unless otherwise stated. Of the 26 subjects enrolled in this study, 13 were randomised to the CON group and 13 were placed the INT group. During the study, one subject of the CON group and two subjects of the INT group deceased due to sepsis. One subject of the INT group was unable to participate in the final examination due to newly diagnosed disease-related severe osteoporosis with fractures. None of these events were related to WBV training. Furthermore, no unwanted side effects were detected. The subjects of the INT participated 27.0 ± 4.1 days (SD) in the WBV training. Training began on the first day of hospitalisation and ended when the subject left the study. Participants left the study individually and not in parallel. Reasons for this are depicted in the study flow chart in Figure 1. No follow-up data was available once subjects left the study.
Descriptive data of the patients including clinical baseline parameters, diagnosis, therapy at baseline and length of stay are provided in Table 1. At baseline, there were no significant differences between the CON group and the INT group. Physical activity was not observed to differ between the two groups. No data on the perceived exertion during the training sessions was collected. Because of the nature of the training schedule, the characteristics of the single training sessions for each subject were extremely individual and each subject raised the respective intensity self-dependently. The training schedule is shown in Supplementary Table 1.
Muscular capacity
The maximum torque at 180°/s extension was observed to decrease from 81.90 ± 28.54 Nm to 73.90 ± 24.50 Nm in the CON group and increased from 78.10 ± 37.72 Nm to 88.60 ± 36.39 Nm in the INT group (p=0.07). At 300°/s extension, the maximum torque in the CON group was observed to decrease from 75.85 ± 31.42 Nm to 66.50 ± 28.02 Nm and increased from 78.11 ± 7.72 Nm to 88.59 ± 36.39 Nm (p=0.09) in the INT group.
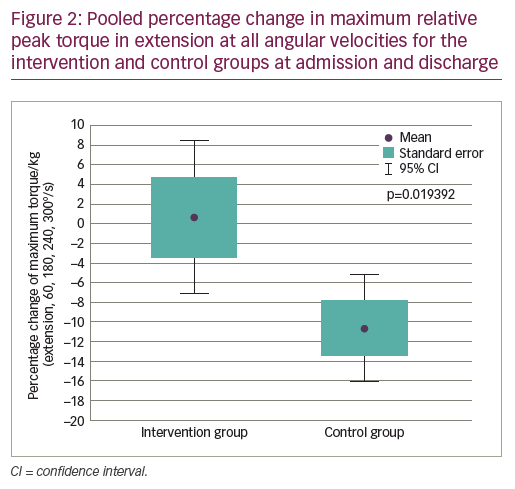
A significant reduced relative peak torque at 60°/s extension was found in all subjects (p=0.04). A decrease from 144.93 ± 34.32 Nm/kg to 137.02 ± 38.52 Nm/kg was found in the CON group compared with a decrease from 152.43 ± 56.04 Nm/kg to 146.20 ± 36.00 Nm/kg in the INT group. A positive trend of WBV training on the relative maximum peak torque at 240°/s extension was observed (p=0.08). The relative maximum peak torque was observed to decrease from 93.39 ± 31.31 Nm/kg to 81.54 ± 32.91 Nm/kg in the CON group and was observed to increase in the INT group from 88.62 ± 37.26 Nm/kg to 98.49 ± 32.28 Nm/kg. Pooling all data on the maximum relative peak torque in extension at all angular velocities, we identified a significant positive effect of the intervention in the INT compared to the CON (p=0.019) as can be seen in Figure 2.
The intervention did not have a significant effect on muscular endurance, number of repetitions, or power. A significant decrease in the power in extension was observed in both the CON and the INT groups (p=0.002). A decrease from 98.90 ± 39.87 J/s to 73.06 ± 37.03 J/s was observed in the CON group, whereas a decrease from 96.00 ± 55.59 J/s to 90.91 ± 45.38 J/s was found in the INT group. A decrease in the power in the flexion was found in the CON group (36.8 ± 27.22 J/s to 26.2 ± 21.62 J/s), and in the INT group (31.44 ± 28.29 J/s to 25.37 ± 15.58 J/s) (p=0.004).
Six-minute walk test
The intervention did not have a significant effect on the covered distance in the 6MWT (p=0.13). A significant reduction in the covered distance was observed in both the CON and the INT group (p=0.004). A decrease from 537.23 ± 117.72 m to 463.94 ± 166.45 m was found in the CON group and a decrease from 562.27 ± 106.72 m to 403.61 ± 235.18 m was found in the INT group.
Health-related quality of life
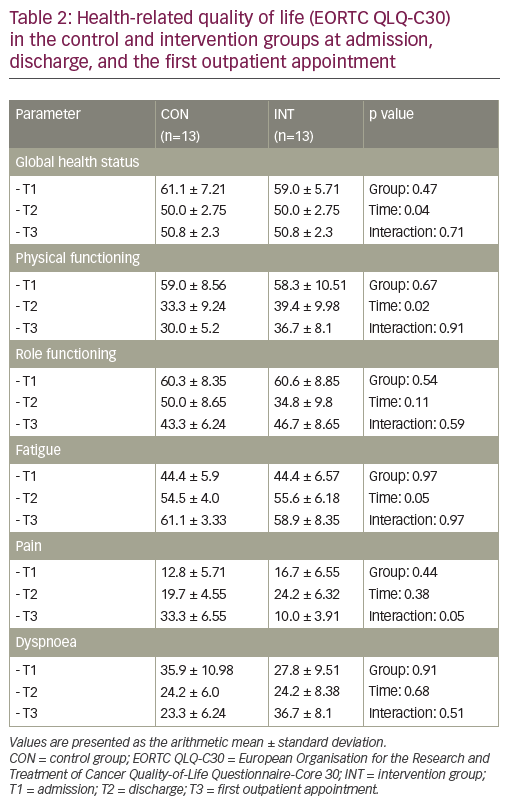
Table 2 depicts results from the HRQOL questionnaire. The general HRQOL significantly declined in all patients (p=0.04). Furthermore, a significant time effect was found for the physical function of patients (p=0.02) and a positive trend was observed for fatigue (p=0.05). A positive trend of the intervention on pain (p=0.05) was also found. In the CON group, a continuous increase in pain from admission to the first outpatient appointment was found. In the INT group, an increase in pain was observed only during inpatient stay. The pain was then observed to decrease until the first outpatient appointment and was subjacent to the value measured at admission. No further significant effects regarding other aspects (physical functioning, role functioning, fatigue, dyspnoea) of the questionnaire were reported in the patients.
Analysis of the training logs
Six complete training logs from patients in the CON group and 10 training logs from patients in the INT could be used for analysis. The frequency of physiotherapeutic treatment significantly differed amongst the groups (p=0.005). On average, subjects of the CON group had physiotherapeutic treatment on 73% of inpatient days and patients of the INT group were found to have treatment on 54% of inpatient days. Physiotherapeutic treatment was applied heterogeneously between the two groups. The frequency of bicycle ergometer use did not significantly differ between the CON and the INT groups (p=0.36). On average, subjects of the CON group used their bicycle ergometer 55% of inpatient days and patients of the INT group were found to use it on 42% of inpatient days.
On the basis of the training log data, the overall attendance rate was 83%. Subjects of the INT group participated in an average of three training sessions per week. No unwanted side effects due to WBV training were reported. The median lowest used intensity of WBV training was Programme 1, the respective highest median used intensity was Programme 18.5.
Intervention satisfaction
Subjects of the INT group were generally satisfied with the intervention, particularly regarding the duration of each training session. The subjects reported the intervention to be enjoyable, safe and recommendable. According to the questionnaires, the most important barriers for using the device were sickness and a lack of motivation related with the medical therapy. The subjects mentioned the easy handling of the device, the low time expenditure and the wide range of possible intensities as the top advantages of the intervention.
Discussion
To the best of our knowledge, this study is the first to implement WBV training along with classic physiotherapy during inpatient stay for patients undergoing allogeneic HSCT. There were no significant differences between the intervention and control groups at baseline.
Furthermore, no unwanted side effects of WBV training were detected. The overall compliance with WBV training was 83%. Subjects in the INT group were required to undergo WBV training 3 days per week. This high compliance is quite remarkable, as the intervention was irregularly supervised and patients with cancer tend to cancel participation in a movement-related intervention during an inpatient stay.15,36 Supervision of the intervention on a regular basis may result in an even higher compliance with more profound effects.
We observed no significant effects of WBV training in addition to physiotherapy during inpatient stay in patients undergoing allogeneic HSCT compared with classic physiotherapy alone on the functional endurance capacity and HRQOL. However, the maximum relative peak torque and pain experienced were observed to improve in the INT compared to the CON, supporting evidence for the effectiveness of the intervention. Pooling the maximum relative peak torques in extension at all measured angular velocities, we identified a significant positive effect of the intervention in the INT compared to the CON (p=0.019). In previous studies, a considerably reduced muscular capacity of the lower extremities has been reported in subjects compared with healthy controls.37,38 Rees et al. found a significantly raised maximum torque at 60°/s extension after 2 months of progressive WBV training using an identically constructed device in older, healthy but untrained subjects.37 In our study, subjects in both the INT and CON groups experienced a decline in the maximum torque in extension, although this reduction was observed to be less in the INT group.
Positive effects following 6 weeks of progressive WBV training with a predominantly vertical vibrating device has been reported in elderly institutionalised subjects.39 In comparison to the intervention in this study, Bautmans et al. used a higher frequency (30–50 Hz). Furthermore, in their study, subjects in the intervention group raised their maximum torque and power at 60°/s extension to approximately 50%.39 Increased efficacy in the enhancement of the muscular capacity of lower extremity musculature has been demonstrated using a predominantly vertical vibrating device.21,22 However, the risk of unwanted side effects appears to be lower for side alternating devices, particularly without regular supervision;40 we selected a side alternating device primarily for this reason. The results of our study confirmed the lack of limiting side effects or overall side effects.
The performance of subjects in the INT group was observed to improve in the final isokinetic testing, reaching significance by pooling all data on the maximum relative peak torque in extension at all angular velocities. The intervention did not significantly affect the covered distance in the 6MWT (p=0.13), although, in both the CON and the INT groups, a significant reduction of the distance covered from the initial test to the final test was found. The subjects in both of the study groups investigated were found to have reduced baseline values compared with previous studies on healthy middle-aged subjects.41,42 At discharge or 40 days following HSCT, the subjects in our study demonstrated comparable values in the 6MWT compared with a previous study on patients with cancer.43
The data obtained from our patients for 6MWT at admission are most comparable with those of Wiskemann et al., who treated patients undergoing allogeneic HSCT with strength and endurance training 4 weeks prior to admission until 6–8 weeks after discharge.44 Upon discharge, subjects that underwent WBV training demonstrated a significantly smaller reduction of the covered distance in 6MWT compared with patients in the CON group. In the study performed by Wiskemann et al., subjects in the INT group commenced the intervention 4 weeks before admission, performed more exercise and completed endurance training that optimally achieved a positive effect in the 6MWT. Apparently our WBV training did not improve the functional endurance capacity.
Data from the EORTC QLQ-C30 show that the general HRQOL and physical function significantly declined in all patients. The values in our study were considerably lower than those reported at baseline in healthy individuals.45,46,47 The intervention was found to have a positive trend regarding an effect on pain in the patients in this study. In the CON group, a continuous increase in pain from admission to the first outpatient appointment was observed, while in the INT group an increase in pain was reported during the inpatient stay and decreased until the first outpatient appointment to a value similar to that measured upon admission. A possible analgesic effect of the application of vibrations has been previously reported, but it appears questionable that such an effect can be achieved beyond the intervention phase such as observed in our study.48 The fact that no further significant effects regarding the other aspects (physical functioning, role functioning, fatigue, dyspnoea) of the questionnaire were reported could be interpreted as the intervention seems to be no additional burden for the patients. Our data are comparable to those of Wiskemann et al. that reported subjects in the INT group to have a significantly better physical function compared with those in the CON group. Furthermore, a reduction in pain following discharge was reported, which is in line with our findings.44 Other studies did not find any effects of a movement-related intervention on the self-reported physical function of patients with cancer during or after chemotherapy measured using the EORTC QLQ-C30, and independently of the effectiveness of the intervention.49,50
We found a significant difference regarding the frequency of physiotherapeutic treatment. Subjects in the CON group were found to have more physiotherapeutic treatments than in the INT group. This factor may have contributed to the lack of significant positive effects of the intervention in the isokinetic measurement of the muscular capacity. This assumption cannot be confirmed due to the lack of data regarding the content of each physiotherapeutic treatment.
Subjects in the INT group were generally satisfied with the intervention, particularly regarding the duration of each training session, enjoyment associated with use of the device and safety. Furthermore, patients that underwent WBV training reported that they would further recommend training. Some of the most favourable characteristics of the device were its simple handling, minimal time required, broad variety of training parameters and potential preservation of muscular capacity. These represent potential advantages of an intervention with WBV training within this specialised setting and emphasize the importance of structured planning considering the specific basics of the therapeutic-medical training theory.26
A factor that may have contributed to an underestimation of the positive effects of the intervention on the muscular capacity may be due to the significant divergences between the preset frequency and the actual applied frequency between -20% and -27% in both devices. Such large divergences signify a different stimulus that may lead to contrasting effects.19,20 Frequencies between 20 and 30 Hz are presumably most effective in increasing the muscular capacity of the musculature of the lower extremities.51 Therefore, the assumed effective frequency ranges cannot be applied and fail to elicit positive effects.52 On the basis of the measurements of the applied frequencies of the devices used in this study, subjects in the INT group used a maximum frequency of 20 Hz, which differed to the maximum frequency provided by the manufacturer (25 Hz). Therefore, the assumed effective frequency range was applied only at the lower end and was less substantially used.
The newly developed training schedule may be an additional factor that may have contributed to an underestimation of the positive effect of the intervention. Although the device was easy to use, the effectivity of the device requires thorough evaluation. Maybe the amplitude of the applied vibrations should be the main progressive parameter and not the frequency.
Our study had several limitations. First, the missing data regarding the exact composition of physiotherapeutic treatments and the use of the bicycle ergometer in all subjects might have confounded the observed relationship between the intervention and the outcomes. In addition, the study is limited by its small sample size and was not blinded at all, because it was obvious that a subject was a member of the INT as the device for WBV training was located in their room. Regarding the missing training logs, we had the problem that some subjects were too tired to fill out the log most of the time and unfortunately some of the subjects of the INT took their training logs home and we were not able to get them back. As such, the self-dependent used training logs might contain unreliable data.
Conclusion
For the first time, we demonstrated that WBV training can be successfully implemented as a supportive therapy for patients undergoing allogeneic HSCT. Additionally, WBV training represents a safe and effective option for the maintenance of the muscular capacity of the musculature of the lower extremities. The intervention was widely accepted by the patients, physicians and nursing staff as it fit well to daily hospital operations. Future studies should focus on ideal training parameters and their progression and optimal control of confounding factors such as physiotherapeutic treatments. Besides this, haematopoietic parameters should also be considered.


