Adolescents and young adults (AYAs) are defined as those individuals between the ages of 15 and 39 years.1 AYAs with cancer are considered a vulnerable group, in large part due to psychosocial challenges in this population, including lack of insurance, low rates of clinical trial enrollment, issues pertaining to independence, and concerns about body image and fertility. The resulting delays in seeking appropriate medical care, delays in diagnosis, and subsequent compliance issues during treatment complicate medical management of cancer among AYAs.2–5 The most recent US Surveillance, Epidemiology, and End Results data indicate less survival improvement in AYAs with cancer compared with children and older adults.6
Hodgkin’s lymphoma (HL) is the most common cancer observed among AYAs.6 There is a slight overall male predominance in this age group, with a male:female ratio of 1.2.6–9 Prior history of infection with Epstein–Barr virus (EBV) has been associated with an increased risk of HL.10 Among AYAs, however, molecular studies show that EBV is related to HL in only a minority of cases and that it is unlikely to play a major etiologic role.11,12 The most common histological subtype of HL among the adolescent and young adult (AYA) population is nodular sclerosing classical HL, occurring in 50–80 % of patients.7–9,13,14 Over the past decades, the prognosis of HL has dramatically improved,15 but the optimal treatment of AYA patients remains undefined and patients continue to be treated on many different regimens with either pediatric or adult protocols. We will examine available literature regarding outcomes for the AYA population and discuss the therapy-related long-term sequelae.
Studies Examining Adolescent and Young Adult Outcomes
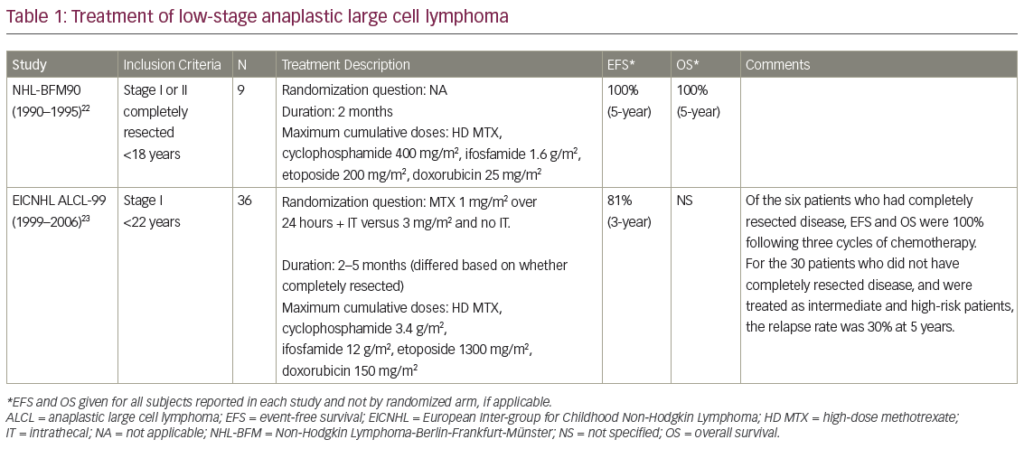
Studies focusing specifically on AYAs diagnosed with HL are scarce. Reviewing the literature, we found eight studies, and their main characteristics are summarized in Table 1. A UK study analyzed adolescents diagnosed with HL between 1970 and 1997 who received treatment with adult-type protocols.16 The OS at 5 and 20 years was 90% and 84% for stage I-IIA HL and 72% and 54% respectively for more advanced disease. However, the event-free survival (EFS) at five and 20 years was 59 % and 52 % in stage I–IIA disease, falling to 41 % and 31% in more advanced disease. The authors highlight that EFS is a more reliable measure of treatment efficacy than OS.
To view the full article in PDF or eBook formats, please click on the icons above.