
Early-onset lung cancer is typically defined as occurring in individuals aged 18–50 years, although there is no universally accepted definition.1–3 This entity, though rare, poses unique diagnostic and therapeutic challenges. This article synthesizes current evidence on the unique features and management challenges of lung cancer in young adults, spanning epidemiology, risk factors, clinical behaviour, histopathology, molecular alterations, therapeutic approaches and survivorship issues (Figure 1).
Figure 1: Key aspects of lung cancer in young adults
Epidemiology and risk factors
Lung cancer is rare among young adults compared with older populations, constituting less than 5% of diagnoses globally in patients aged ≤40 years.4 However, there is no universally accepted definition for the upper age limit of ‘young‘ or ‘early onset’; some studies use a cutoff of 40 years, while others define it as under 35 years of age, contributing to variability in reported incidence and outcomes. The National Cancer Institute (NCI) defines early-onset cancer as a diagnosis occurring under the age of 50.5 A retrospective analysis by Sacher et al. showed that patients under 50 years had a 59% increased likelihood of harbouring actionable genetic alterations, suggesting this age as a potential diagnostic threshold.2
The incidence of early-onset lung cancer varies geographically.1,6–10 Air pollution, cultural habits and environmental exposure are likely to contribute to this variation. Although cases have been reported in individuals as young as 14 years, the median age at diagnosis in younger cohorts typically ranges between 36 and 39 years.1,6 The variability of incidence is shown in Figure 2.1,6–10
Figure 2: Reported incidences of lung cancer in young adults in different regions1,6–10
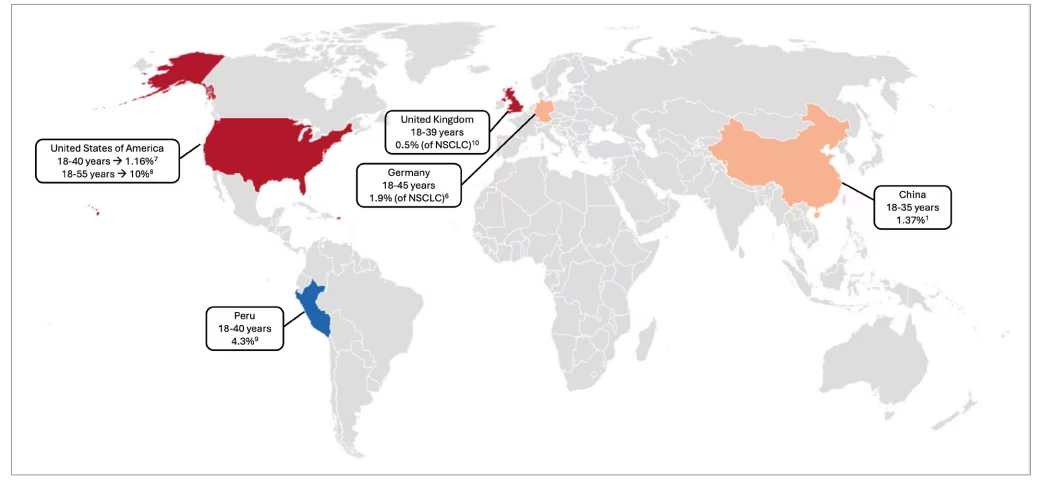
NSCLC = non-small cell lung cancer
While the overall incidence of lung cancer in young adults has declined over recent decades (see Figure 3), this trend is attributed mainly to decreasing tobacco use due to widespread public health interventions, including smoking cessation programmes, advertising restrictions and taxation.11 For instance, youth smoking rates in the USA have declined from over 28% in the 1990s to under 5% in recent years.12 Other contributors to the downward trend in incidence include improved air quality regulations and reduced occupational exposure to carcinogens.13–15
Figure 3: Trends in lung cancer incidence in young adults11
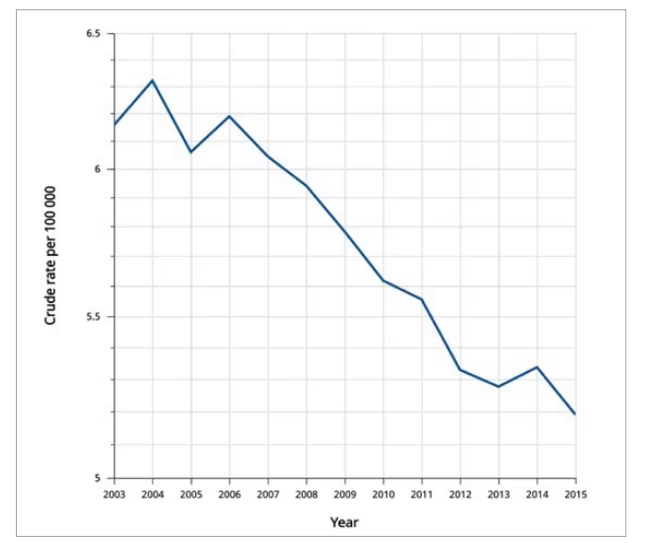
Data source: Global Cancer Observatory: Cancer over time, from the International Agency for Research on Cancer/World Health Organization (IARC/WHO). Reprinted from World Health Organization International Agency for Research on Cancer. Trends in cancer incidence and mortality rates. Available at: https://gco.iarc.fr/overtime (accessed: 12 July 2025)11
Lifestyle habits
Tobacco smoking remains the primary risk factor for lung cancer; however, its prevalence is lower among younger patients than in older cohorts. In young adults, smoking prevalence ranges from 15% to 71%, compared with 34% to 83% in older adults.6,16,17 The roles of vaping and cannabis remain under investigation. Although cannabis is frequently co-used with tobacco, complicating risk stratification, some studies suggest a potential association between cannabis use and more aggressive disease phenotypes in young adults.17,18
Another modifiable cancer risk factor is obesity. A meta-analysis reported an inverse association between excess body weight (body mass index [BMI]≥25 kg/m²) and lung cancer incidence, particularly among smokers (relative risk=0.63).19 The so-called ‘obesity paradox’ in smokers that suggests that individuals with higher BMI may experience lower disease incidence and improved outcomes remains a topic of ongoing debate and controversy.20
Environmental and occupational factors
Environmental and occupational exposures are also important contributors, especially given the lower prevalence of traditional risk factors like tobacco use in this population. Air pollution, radon gas and carcinogens such as arsenic and cooking fumes have been implicated in lung cancer risk.
Ambient air pollution is a well-established carcinogen. Fine particulate matter (PM2.5), nitrogen dioxide (NO2) and ozone are associated with increased lung cancer risk, with a powerful effect observed in younger individuals. A recent meta-analysis found that PM2.5 exposure increased the relative risk of lung cancer by 9–16% per 10 μg/m³ and the risk rose to 63% among individuals under the age of 50.21 People residing in urban areas have been found to face a greater risk of developing lung cancer compared with those living in rural settings, likely due to higher levels of air pollution and environmental exposures.22 Diesel motor exhaust, a major contributor to worldwide urban air pollution, consists of a complex mix of organic and inorganic substances in gaseous and particulate forms.23 Prolonged exposure to diesel motor exhaust has been linked to an elevated risk of lung cancer, especially with squamous cell carcinoma.
As a naturally occurring radioactive gas that accumulates in poorly ventilated indoor environments, radon has been shown to increase lung cancer risk in a dose-dependent manner, with a 16% increase in relative risk per 100 Bq/m³.24 This is especially relevant in younger individuals who may spend more time indoors during developmental years.25,26 Additionally, new residential buildings, occupied mainly by younger people, including children and pregnant women, carry a higher risk of radon exposure than older buildings. Given the increased vulnerability associated with early-life exposure, these findings raise concerns about a potential future rise in radon-induced lung cancer among younger populations.25
Second-hand smoke, particularly during critical developmental periods such as childhood and adolescence, contributes to long-term lung cancer risk.27,28 Involuntary inhalation of tobacco smoke introduces numerous carcinogens, including polycyclic aromatic hydrocarbons and nitrosamines, which can cause long-term molecular damage to lung tissues. Studies have shown that individuals exposed to secondhand smoke in early life have a markedly increased risk of developing lung cancer later, with some reporting odds ratios as high as 3.9, highlighting the importance of developmental windows of vulnerability.27,28 Given that secondhand exposure is both preventable and common in household and social settings, especially in low-regulation environments, reducing early-life exposure remains a critical public health goal in the prevention of early-onset lung cancer.
Occupational and household exposures also merit consideration, even in younger patients with shorter exposure durations. Carcinogenic agents such as asbestos, silica and arsenic are implicated in lung carcinogenesis.29 Asbestos remains a significant concern due to its synergistic effect with tobacco smoke, its established role in promoting non-small cell lung cancer (NSCLC) and mesothelioma.30 Besides occupational exposure, household exposure of family members or residential exposure from mining or factories can increase the risk.31 Arsenic is a well-established environmental risk factor for lung cancer.32 Globally, millions of individuals are exposed to elevated arsenic levels through contaminated drinking water and food, prompting the WHO to recommend a maximum concentration of 10 µg/L in water to reduce health risks.33
Indoor combustion of biomass fuels such as wood and coal, frequently used for cooking and heating in low- and middle-income countries, can result in substantial exposure to smoke and polycyclic aromatic hydrocarbons in poorly ventilated spaces, thereby increasing lung cancer risk.34,35 This association is supported by evidence showing that greater levels of indoor smoke are significantly correlated with higher lung cancer incidence.36 This risk is particularly concerning for women and children in many low-resource settings, where cultural and economic factors often result in women undertaking domestic duties and children spending more time indoors, leading to disproportionate exposure to harmful indoor air pollutants.34–36
Finally, growing attention is being paid to environmental endocrine-disrupting chemicals (EDCs), such as bisphenol A (BPA), phthalates and pesticide residues, which may interact with hormone and growth factor pathways.37 These agents are widely present in plastics, personal care products and food packaging. They are suspected to influence lung carcinogenesis by mimicking or blocking hormonal pathways, particularly 0estrogen, altering immune function and enhancing susceptibility to mutagenic damage, especially in younger, hormonally active individuals.38
Taken together, these diverse environmental exposures underscore the multifactorial nature of lung cancer in young adults and highlight the need for detailed exposure histories in clinical evaluation and research.
Hormonal factors
Emerging evidence highlights sex-specific differences in young adult lung cancers, with women under 40 years facing a higher incidence compared with men, independent of smoking.2,9,17,39 Hormonal factors, particularly oestrogen, are implicated in this disparity. Oestrogen receptors (ERs), especially ER-β, are expressed in lung tissues, and oestrogen may induce the progression of tumour growth.40 Additionally, higher nuclear expression of ER-β was observed in 67% of epidermal growth factor receptor (EGFR)-mutant cases compared with 37% in EGFR wild-type tumours.41,42 Recent studies also indicate a crosstalk between oestrogen signalling and EGFR receptors in lung carcinogenesis.43 oestrogen triggers tumour angiogenesis through vascular endothelial growth factor (VEGF) and also promotes VEGF-A, a part of the downstream pathway of EGFR.44 Combining the multitargeted tyrosine kinase inhibitor (TKI) vandetanib with the anti-oestrogen fulvestrant enhances its antitumour effect in NSCLC.45 The interplay between oestrogen, genetic susceptibility (e.g. EGFR mutations) and environmental exposures like smoking, where oestrogen may amplify tobacco-related deoxyribonucleic acid (DNA) damage, further complicates the risk profile. Several clinical trials exploring this topic are summarized in Table 1.46–50
Table 1: Clinical trials of hormonal therapy in lung cancer46–50
| ClinicalTrials.gov identifier | Phase | Patient population | Experimental treatment | Hormone receptor assessment |
| NCT0155619146 | II | Postmenopausal women with stage III or IV, EGFR wild or mutant non-squamous NSCLC | mEGFR: gefitinib + fulvestrant EGFR wild: erlotinib + fulvestrant | Not defined |
| NCT0059200747 | II | Postmenopausal women with stage III or IV NSCLC who are treated with four cycles of induction chemotherapy and not progressed | Fulvestrant + anastrazol as consolidation | Correlative tissue analysis |
| NCT0010085450 | II | Patients with stage III or IV NSCLC and stable disease on erlotinib | Fulvestrant+ erlotinib | Oestrogen or progesterone receptor positive |
| NCT0266610548 | II | Postmenopausal women with advanced NSCLC who have progressed on treatment with an ICI | Exemestane | Correlative tissue analysis |
| NCT0166475449 | I | Postmenopausal women with treatment-naïve stage III or IV non-squamous NSCLC | Carboplatin + pemetrexed + exemestane | Not defined |
EGFR = epidermal growth factor receptor; ICI = immune checkpoint inhibitor, mEFGR = mutated epidermal growth factor receptor; NSCLC = non-small cell lung cancer.
Genetic factors and genomic alterations
Genetic and molecular factors play a critical role in early-onset lung cancer. Although a positive family history has been found in only 1.3–4.2% of cases, individuals with an affected first-degree relative have a significantly elevated risk with odds ratio of 3.3 and also 2.6 when any relative is affected.1,51–53 In addition, inherited pathogenic variants in cancer predisposition genes, particularly those involved in DNA repair pathways, have been identified in 4–15% of early-onset cases.54,55 Reflecting the growing recognition of heritable susceptibility, the National Comprehensive Cancer Network (NCCN) recommends germline genetic counselling for selected patients with NSCLC, such as those diagnosed with EGFR T790M mutation.56
In addition to inherited risk, patients with early-onset lung cancer demonstrate a significantly higher prevalence of actionable driver mutations, particularly involving EGFR and anaplastic lymphoma kinase (ALK), supporting the routine implementation of comprehensive molecular profiling at diagnosis.57 In younger populations, the prevalence of targetable driver mutations, including EGFR, ALK and c-ros oncogene 1 (ROS1), reaches 60–70%, substantially higher than in older adults.2,58,59 In the retrospective study from France with 189 patients aged 18–45 years, 40% of the metastatic group had either EGFR, ALK or ROS1 mutation.17 These mutations are particularly enriched among non-smokers, females, younger patients and those with adenocarcinoma histology.60 A retrospective study from Spain with 26,336 patients comparing genetic characteristics between young and older patients with lung cancer demonstrated that patients aged ≤35 years had a higher prevalence of ALK rearrangements and ROS1 mutations than those >35 years. Additionally, patients aged ≤50 years were significantly more likely to harbour ALK translocations and human epidermal growth factor receptor 2 (HER2) mutations, with odds ratios of 7.61 and 5.71, respectively.61
Among oncogenic drivers, EGFR mutations are the most frequently observed oncogenic driver in this age group, accounting for approximately 20–50% of oncogene-addicted tumours followed by Kirsten rat sarcoma viral oncogene (KRAS) alterations (15.1%), serine/threonine kinase 11 (STK11) mutation (10%) and SMARCA4 mutation (7.7%).2,59,62,63 EGFR exon 19 deletions are more common in younger patients.64 A genomic analysis of 421 young Chinese patients aged 20–40 years confirmed the high frequency of ALK rearrangements and reported a higher prevalence of HER2 mutations compared with older patients aged 60–80 years.51 Notably, KRAS G12D, a non-smoker-associated mutation, was more prevalent in patients aged ≤50 years, and the frequency of KRAS G12C increased with age.57 The RET gene and NTRK1 fusion are also enriched in young patients.57
Tumour immunity
Tumour mutation burden (TMB) is mostly low in patients with targetable alterations.57 It usually varies by mutation subtype, with EGFR-mutant tumours typically displaying lower TMB compared to those harbouring KRAS or v-raf murine sarcoma viral oncogene homolog B1 (BRAF) mutations.65 Notably, cannabis users frequently exhibit low programmed cell death ligand 1 (PD-L1) expression and lack targetable oncogenic alterations.17 Several studies showed decreased expression of immune-related genes in the tumour microenvironment, as well as decreased infiltration of immune cells, particularly T cells.52,58 Transcriptomic studies have suggested potential alterations in cellular metabolism pathways and the expression of immune-related genes.51
Clinical presentation and diagnosis
Lung cancer in young adults often presents with nonspecific symptoms. The most frequently reported symptoms in this population include cough (62–72%), dyspnoea (41%) and chest pain (23–52%).66,67 These often mimic benign conditions, leading to diagnostic delays. Approximately 38% of patients also present with extra-thoracic manifestations, such as neurological symptoms due to brain or spinal cord metastases.9 A delayed diagnosis is further compounded by empirical antibiotic treatment prior to definitive work-up. In one study, 39.8% of young patients with small cell lung cancer (SCLC) had received antibiotics for presumed infection, which may have obscured more specific symptoms.67 The median interval from symptom onset to diagnosis has been reported as 61 days, ranging from 1 to 1,076 days.68
Early-onset lung cancer typically presents with more advanced disease; 41–84% were diagnosed at a metastatic stage.1,9,17,39 Similarly, Liu et al. reported that 49.2% of patients had metastatic disease at presentation, with the most common metastatic sites being the pleura (38.7%), bone (35.4%) and lungs (25.8%).1 Notably, 68% of cases exhibited oligometastatic disease, typically involving a single organ. Among lung cancer histologies, NSCLC constitutes a greater proportion of cases in young adults (95%) than in older patients (85%), with adenocarcinoma being the predominant subtype, observed in 45–73% of cases.6,9,17,58 Although small-cell lung cancer is relatively rare in young adults, it tends to exhibit aggressive behaviour when it does occur.6,67
Next-generation sequencing (NGS) has become a critical tool in the diagnosis and management of NSCLC, enabling comprehensive genomic profiling that is particularly valuable in younger patients who often lack traditional risk factors like smoking.69 Since early-onset lung cancer is characterized by a higher prevalence of actionable driver mutations, NGS facilitates the simultaneous detection of common, rare and compound driver mutations, while also identifying germline alterations in cancer predisposition genes, enabling personalized treatment strategies with targeted therapies and informing genetic counselling and family screening. With the better optimized treatment, NGS was associated with better survival outcomes.70
Treatment considerations and outcomes
Despite presenting at more advanced stages, young adults with lung cancer often have better performance status and fewer comorbidities, enabling them to tolerate aggressive treatment regimens.71 While direct evidence from recent large-scale studies on physician preference for treating young adults more intensively is limited, established oncologic principles support offering more intensive therapies to younger, fitter patients.1,72 The Society of Thoracic Surgeons, in its 2025 clinical practice guideline, recognizes a high level of evidence supporting surgical therapy in patients with stage IV NSCLC who are appropriately selected for local consolidative therapy, including pulmonary metastasectomy, although the optimal extent of resection remains an area of ongoing investigation.72 Since young patients have lower morbidities, the chance of being fit for surgical metastasectomy is much higher. In the study of Galvez-Nino et al., from the cohort of 166 patients with early-onset lung cancer, 92% of patients received systemic therapy and 23% underwent surgical resection.9 Overall, in the metastatic setting, local therapy, while primarily intended to improve disease-free survival or facilitate symptom control, should be considered more frequently as an option within a multidisciplinary team discussion.
The availability of targeted therapies has significantly improved the prognosis of younger patients, particularly those with driver mutations. Epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs), ALK inhibitors and ROS1 inhibitors are commonly employed.73–75 These treatments are generally well-tolerated, even with long-term use, making them particularly suitable for younger patients with longer life expectancy.73–75 However, the dermatologic toxicities associated with EGFR-TKIs can have a greater impact on quality of life in this age group.76 Combination regimens in EGFR-mutated NSCLC, such as osimertinib with chemotherapy (platinum plus pemetrexed), improved survival compared with monotherapy, with patients under 65 years appearing to derive greater benefit (HR 0.59 versus 0.68 in older adults).77 For ALK-rearranged NSCLC, lorlatinib offers strong central nervous system protection, with a 5-year PFS rate of 60% and greater benefit in younger patients (HR 0.22 for <65 years).78 In ROS1-rearranged cases, repotrectinib showed better outcomes in patients under 65 years, with an overall response rate of 81%, compared with the 65–75-year-old patients with 67%.79 However, although agents with intense central nervous system penetration, such as lorlatinib, taletrectinib and repotrectinib, are often appropriate for younger patients, they commonly cause unique adverse effects, including cognitive impairment and mood changes, which may significantly disrupt the quality of life in this typically active population.78–80
Immunotherapy, alone or combined with chemotherapy, plays a role in treating metastatic patients without actionable mutations. Although young adults tend to have a lower tumour mutation burden and are more often non-smokers, which may correlate with less responsiveness to immune checkpoint inhibitors (ICIs), some benefits have been observed.81 Given the relatively low PD-L1 expression in many of these tumours and decreased expression of immune-related genes in the tumour microenvironment, the choice of immunotherapy must be individualized.57 A large dataset including 53,719 patients showed that the 2-year survival benefit from ICIs was more pronounced in patients aged 55 years and younger compared with those aged 75 years and older. Notably, ICI-chemotherapy combinations were more frequently administered to younger patients.82 However, in a real-world analysis of patients under 40 years, ICIs were not an independent predictor of improved survival.83
The immune system in younger individuals tends to be more active, which may paradoxically contribute to earlier T-cell exhaustion in the tumour microenvironment. As a result, younger patients may initially mount a more robust immune response, but this may decline more rapidly. Conversely, older individuals experience immunosenescence, a gradual decline in immune function, which may dampen the initial response to immunotherapy but allow for more sustained T-cell activity over time.84 High oestrogen levels of females—such as during the luteal phase or pregnancy—can suppress cell-mediated immunity by reducing CD8+ T-cell activity and increasing regulatory T cells, dampening antitumour responses.40 Oestrogen also upregulates immunosuppressive factors (e.g. PD-L1 and transforming growth factor beta [TGF-β]) and recruits myeloid-derived suppressor cells, contributing to a ‘cold’ tumour microenvironment less responsive to immunotherapy. Conversely, oestrogen may enhance B-cell activity and antibody production, potentially supporting antibody-based therapies like ICIs.40 While both male and female patients benefit from immunotherapy, females tend to derive less benefit compared with males.85
Survival outcomes among young adults with lung cancer vary significantly by the disease stage and molecular profile. Early-stage disease is associated with favourable long-term survival, whereas stage IV disease typically carries a median overall survival of 12–24 months, depending on the treatment strategy and biomarker status.9,17 Favourable prognostic factors include good performance status, presence of actionable mutations and limited metastatic burden.1 However, data from the SEER database suggest that patients under 40 years may paradoxically have worse overall survival compared with older counterparts. Risk factors contributing to this outcome include advanced disease stage at diagnosis, adenocarcinoma histology and lack of health insurance.86 In line with SEER data finding, survival outcomes for patients under 40 years of age was not superior to those of older adults, which may be attributable to more aggressive tumour biology in this age-group.2
Lung cancer diagnosis during pregnancy is highly rare, with a limited number of cases in the literature.87 However, as general oncological practice, since computed tomography, positron emission tomography-computed tomography and scintigraphy should be avoided due to their possible teratogenic effects, safer methods like ultrasound sonography or MRI should be used for tissue sampling and staging.88 Surgery can be performed throughout the pregnancy, but it is safest in the second trimester, and general anaesthesia should be avoided.89 Weekly carboplatin combined with vinca alkaloids or taxanes is considered safe during the second and third trimesters, but pemetrexed and gemcitabine are prohibited due to their teratogenic effects.90 Palliative radiotherapy could be administered with proper abdominal shielding, keeping the safe dose of 0.1–0.2 Gy; however, this option should be considered as the last option.91 ICIs and TKIs are considered teratogenic based on preclinical data.92,93
Long-term follow-up and survivorship
Young patients with lung cancer face distinct psychosocial and reproductive health challenges, including fertility preservation and sexual dysfunction, which must be addressed as part of a comprehensive treatment plan.16 These factors highlight the need for a personalized diagnostic and therapeutic approach. Chronic symptoms such as fatigue, dyspnoea and pain may persist long after treatment.90 In contrast, the psychological burden, such as anxiety about recurrence and concerns about relationships or future planning, is often more profound in this population.94,95 Early referral to fertility specialists is recommended before initiating systemic therapy.96
Therefore, survivorship care plans should integrate mental health support, lifestyle counselling (e.g. smoking cessation, exercise and nutrition) and surveillance for second malignancies. The increasing use of TKIs and ICIs introduces novel long-term toxicity profiles that are not yet fully understood, particularly in younger individuals who may require prolonged treatment.97,98 Close collaboration between oncologists and primary care providers is essential for coordinated, long-term follow-up. Reproductive health considerations are critical, as chemotherapy, radiation, ICIs and TKIs can impair fertility.99 Up to 50% of men may develop azoospermia, and up to 50% of women may experience amenorrhoea following cytotoxic chemotherapy; preclinical evidence suggests potential gonadotoxicity of programmed cell death protein 1/PD-L1 inhibitors.100,101 TKIs may impair corpus luteum function and alter steroidogenesis.93 EGFR-TKIs may lower testosterone and dehydroepiandrosterone in patients with NSCLC. BRAF and RET inhibitors may compromise male and female fertility, and they should be avoided during pregnancy and have a follow-up post-treatment.102,103
Beyond medical concerns, young patients face career disruption, financial strain and increased psychological stress, highlighting the need for multidisciplinary support, including psycho-oncology and social work.104–111 Financial toxicity, especially pronounced in adolescents and young adults, arises from the economic burden of cancer treatment before achieving financial independence or career stability.107,108,112 This includes direct costs like co-pays and non-reimbursed therapies, as well as indirect costs such as lost wages and reduced productivity.113,114 Long-term survivors among young adults often encounter enduring challenges related to treatment sequelae and overall quality of life.109–111,115 Surveillance strategies should be adapted to account for longer life expectancy and the risk of late toxicities, such as chemotherapy-induced cardiotoxicity or TKI-related interstitial lung disease. Comprehensive, age-appropriate survivorship plans are essential to optimize health outcomes and quality of life in this unique population.
Discussion
Early-onset lung cancer, though uncommon, presents a distinct clinical and molecular profile that differs from lung cancer in older adults. Young patients often lack traditional risk factors such as long-term tobacco exposure and instead exhibit a higher frequency of oncogenic driver mutations, including EGFR, ALK, ROS1 and HER2. In parallel, environmental factors require greater scrutiny. Unlike the tobacco-driven carcinogenesis predominant in older patients, early-onset lung cancer may be linked to early-life exposure to radon, second-hand smoke, air pollution, biomass combustion and endocrine-disrupting chemicals. However, current evidence remains limited, and further epidemiological studies are needed to clarify these associations.
The high prevalence of targetable molecular alterations underscores the importance of comprehensive genomic profiling at diagnosis, as targeted therapies can substantially improve clinical outcomes in this population. Despite recent therapeutic advances, several controversies and challenges remain. The overall prognosis of early-onset lung cancer is not necessarily better than that of older patients, mainly due to delayed diagnosis and the lack of screening eligibility for younger populations. However, current lung cancer screening is solely focused on smoking exposure and age categories, and more evidence is required to develop a standardized lung cancer screening in this patient population.
Additionally, intensified treatment regimens, while potentially more effective, may carry unique burdens in younger patients, particularly concerning quality of life, neurotoxicity and long-term adverse events such as endocrine dysfunction and fertility impairment. This highlights the need for age-sensitive counselling, survivorship planning and multidisciplinary support during and after active treatment. From a clinical perspective, treatment decisions in early-onset lung cancer must balance aggressive disease control with quality-of-life preservation. The longer expected lifespan in these patients amplifies the long-term consequences of treatment-related toxicities, psychosocial stress and impaired life milestones. Therefore, integrating fertility preservation, mental health support and rehabilitation into routine care is essential.
Finally, the psychosocial burden of a cancer diagnosis in young adulthood, including disruptions to education, employment, family planning and identity formation, should not be underestimated. These aspects must be considered in both research and clinical frameworks to improve patient-centred outcomes.
Future directions and research needs
Due to the rarity of lung cancer in young adults, most data come from retrospective analyses or subgroup findings in broader clinical trials, limiting age-specific insights into treatment efficacy and safety. Despite often being eligible for trials, young patients remain underrepresented in targeted research. Prospective studies, clinical trials and collaborative registries are needed to clarify this population’s unique biological and clinical features. Given that most young adult patients with lung cancer are non-smokers and ineligible for standard screening, new biomarkers and predictive tools based on clinical and familial history are essential to improve early detection, reduce misdiagnosis and prevent unnecessary treatments. Table 2 summarizes ongoing clinical trials designed for young adults with cancer.116–121
Table 2: Ongoing clinical trials recruiting young adults with lung cancer116–121
| ClinicalTrials.gov identifier | Type | Trial name | Age group | Intervention |
| NCT05265429116 | Observational | Biology of Young Lung Cancer Study: The YOUNG LUNG Study | 45 years and younger | Genetic data and specimen collection |
| NCT06397651117 | Interventional | A Randomised Controlled Trial to Evaluate the Impact of Complement Theory’s Live 1:1 Exercise Coaching and Personalised Digital Application on Cancer Survivors’ Cost of Care | 21–64 years | Behavioural: exercise coaching and personalised digital application |
| NCT01590069118 | Interventional | Aerosolized Aldesleukin in Treating Patients With Lung Metastases | 12–50 years | Aerosolized aldesleukin |
| NCT04551378119 | Observational | The Effect of COVID-19 Pandemic on Adolescent and Young Adult Cancer Patients and Survivors | 18–39 years | Quality-of-life assessment |
| NCT04577599120 | Interventional | Lung B.A.S.E.S. 4 Life Mobile Low-dose Computed Tomography (LDCT) Screening: Ages 40-54 | 40–54 years | Mobile low-dose computed tomography screening |
| NCT05131815121 | Interventional | The BurnAlong Pilot Study for Adolescent and Young Adult Cancer Survivors | 18–39 years | Behavioural: virtual group–based physical activity |
Conclusion
Early-onset lung cancer is associated with high molecular alterations, delayed diagnosis and significant psychosocial impact on patients. Although rare, its burden is considerable, affecting patients during critical life stages. While advances in targeted therapies and immunotherapies have expanded treatment options, a critical need remains for dedicated research in patient-centred and personalized screening, age-specific clinical trials and comprehensive survivorship care. A multidisciplinary, patient-centred strategy alongside innovations in early detection and raising awareness is key to improving outcomes and quality of life for this vulnerable group.










