Pancreatic cancer (PC) is the tenth most common cancer in 2024, with 66,440 new cases and 51,570 deaths.1,2 Globally, the prevalence varies from 10/100,000 cases in the Americas and Europe to 0.9/100,000 cases in South Central Asia and most of Africa.3 Currently, it has the third-highest mortality:incidence ratio, with an increasing death rate of 0.23% annually, paralleling the increased incidence, which predisposes it to be the second leading cause of cancer death by 2030.1 Its aggressive nature, late-stage diagnosis and limited treatment options result in a 2–9% 5-year survival rate.4
A recent time-trend analysis indicated a rising incidence of PC in younger women and men, particularly in women aged 15–34 years.5 While 90% of cases with PC occur sporadically, 5–10% are linked to hereditary and familial predisposition syndromes.4,6 Pancreatic ductal adenocarcinoma is the most prevalent type of PC, making up approximately 95% and is considered one of the most fatal malignancies globally, with a 5-year survival rate of approximately 13%.7–9
Diagnosis and treatment disparities represent a global challenge that worsen the outcomes.10,11 Black individuals experience a 50–90% higher incidence, with rates of 15.9 per 100,000, followed by White with 13.4, Hispanic with 12.2 and Asian with 10.3 per 100,000, reflected in higher mortality rates among Black individuals and approximately 50,000 deaths annually.12,13 These differences are influenced by a combination of lifestyle factors, socioeconomic status, living conditions and genetic predispositions.14 Addressing their impact on PC outcomes is vital for social justice, reducing the cancer burden, improving population health and designing healthcare systems and initiatives that promote equitable survival outcomes.11,15
Owing to the rarity of PC, several aspects remain poorly understood. This article aims to explore emerging trends in PC pathophysiology, molecular characteristics and novel treatment approaches. We seek to identify gaps in the literature to guide future research.
Pathophysiology and molecular biology
Precursor lesions and cell of origin
The endocrine gland constitutes only 10% of the pancreas, while the exocrine gland constitutes the remaining 90%, comprising 85% acinar cells and 5% ductal cells.16 Pancreatic ductal adenocarcinoma can begin with four precancerous lesions (PLs) that arise from ductal or acinar cells. These PLs differ in their clinical pathology and genetics and are categorized into pancreatic intraepithelial neoplasia (PanIN), intraductal papillary mucinous neoplasm, mucinous cystic neoplasm and pancreatic intraductal tubulopapillary neoplasm.17 There is limited understanding in the literature about PLs and early-stage disease, which could considerably increase survival rates by easing early detection and treatment. The PLs of pancreatic ductal adenocarcinoma are presented in Supplementary Table 1.
Molecular signalling pathways and tumour microenvironment
Although many signalling pathways are known to be involved in pancreatic ductal adenocarcinoma progression, there is no literature on how these pathways interact to evade immunity, tumourigenesis and metastasis. Supplementary Table 2 highlights the main signalling pathways involved in pancreatic ductal adenocarcinoma progression.
The tumour microenvironment (TME), an evolving niche of cellular and acellular components, interacts with cancer cells to meet their nutritional and metabolic needs (Figure 1).18 It plays a crucial role in pancreatic ductal adenocarcinoma pathogenesis, and Supplementary Table 3 summarizes the TME components of pancreatic ductal adenocarcinoma.
Figure 1: Tumour microenvironment and the therapeutic implications
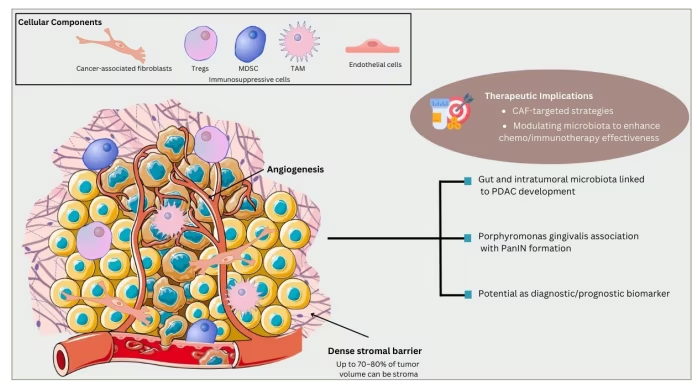
Figure created with Canva.com.
CAF = cancer-associated fibroblast; MDSC = myeloid-derived suppressor cell; PanIN = pancreatic intraepithelial neoplasia; PDAC = pancreatic ductal adenocarcinoma; TAM = tumour-associated macrophage; Tregs = regulatory T cells.
The intratumour microbiome is a crucial TME component that influences carcinogenesis, progression and therapy responses, and has potential as a diagnostic and prognostic biomarker. The gut microbiome, which comprises bacterial, fungal and viral species, contributes to the development of pancreatic ductal adenocarcinoma. Although the pancreas is considered sterile, the development of the intratumoural microbiome, in addition to changes in the oral and faecal microbiota, is linked to pancreatic ductal adenocarcinoma progression.19 Furthermore, the gut–oral microbiota has been linked to the intratumour microbiome, influencing nutrient use and suppressing antitumour immunity, creating a favourable TME.20 Microbiome perturbation leads to persistent pancreatic inflammation, promoting pancreatic ductal adenocarcinoma through immune system changes via inflammatory cytokines and immune cells, or through metabolic alterations in the TME.19 A Mendelian randomization study identified 20 gut micro-organisms associated with PC, including species from p_Bacteroidetes, p_Firmicutes and p_Proteobacteria.21 Some bacteria also secrete carcinogens. For example, Porphyromonas gingivalis, an oral pathogen, has been linked to pancreatic ductal adenocarcinoma by activating transforming growth factor beta (TGF-β) signalling and enhancing PanIN lesion growth in mouse models. This may explain the higher risk of pancreatic ductal adenocarcinoma in patients with periodontal disease.22 Despite this progress, the specific mechanisms of the gut microbiome in pancreatic ductal adenocarcinoma remain unclear.
Diagnosis and screening
Since PC is a disease with a poor prognosis, there is an urgent need to develop minimally invasive and effective diagnostic tools for early-stage PC detection, in addition to the advanced tools required for staging and management.23,24 Currently, there are no screening programmes for PC owing to its low occurrence and lack of cost-effective, non-invasive methods. However, targeting high-risk groups could be cost-effective and have a positive survival impact.25
Imaging techniques for diagnosis
-
Computed tomography (CT): A cornerstone for PC diagnosis, with >90% sensitivity for detecting solid pancreatic nodules but 77% for small (<2 cm) tumours. PC requires multiphase imaging with iodinated contrast (1.5 mL/kg at 4–5 mL/s).26
-
Endoscopic ultrasound (EUS): Essential for staging, biopsy and assessment of vessel involvement. It is preferred for tissue sampling when used with fine-needle aspiration (FNA). The sensitivity of EUS-FNA ranges between 54% and 74%, indicating that it is not highly accurate for ruling out neoplasms. Additionally, there is a small risk of neoplastic seeding associated with EUS-FNA.27
-
Magnetic resonance imaging (MRI): Provides superior soft-tissue contrast, and advanced techniques (e.g. diffusion-weighted imaging) are ideal for evaluating ductal strictures and tissue characteristics. It is less invasive but less sensitive than EUS for sub-centimetre lesions.28
-
Endoscopic retrograde cholangiopancreatography: Used prior to surgery to relieve obstruction by stenting for hyperbilirubinaemia.27
-
Positron emission tomography-CT: Has limited routine use due to 78% false-positive and 9.8% false-negative rates, although it is helpful for staging localized, non-metastatic tumours.
Biomarkers for diagnosis and screening
Although numerous biomarkers aid in early detection, they have not yet provided sufficient evidence to improve survival outcomes.29 The two most important biomarkers currently used in clinical practice are carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen (CEA).30,31
Carbohydrate antigen 19-9 and carcinoembryonic antigen
CA19-9 is the most widely used biomarker for PC detection, but its accuracy is limited by false positives (e.g. inflammatory conditions) and false negatives (e.g. Lewis antigen-negative individuals).32,33 To improve diagnostic precision, recent studies have explored the combination of CA19-9 with TIMP1, LRG1 and cfDNA methylation, achieving an area under the curve (AUC) of 0.92.34 Postoperatively, rising CA19-9 levels can indicate recurrence, even in the absence of radiological evidence.35 Additionally, its involvement in PC progression and angiogenesis suggests its potential as a therapeutic target.36
CEA improves diagnostic accuracy when combined with biomarkers, such as interleukin-8 (IL-8) and carcinoembryonic antigen-related cell adhesion molecule 6 (CEACAM6) (AUC: 0.89).37 It may also aid in diagnosing CA19-9-negative cases, although further validation is required.38 Supplementary Tables 4 and 5 summarize recent studies on biomarkers of PC.
TP53 and KRAS
Mutations in TP53, a key tumour suppressor gene, are prevalent in PC, affecting carcinogenesis and therapy resistance by disrupting cell-cycle regulation and apoptosis.39,40 TP53 also modulates the TME and preneoplastic lesion growth, making it a crucial target for further study.39
KRAS mutations occur in 90–95% of PC cases and are linked to poor survival and early metastasis.41 Combining KRAS mutations with epigenetic markers improves the diagnostic performance (AUC: 0.933; sensitivity: 90%; specificity: 95%).42 KRAS also influences metabolic reprogramming, including glutamine addiction, contributing to chemoresistance.43 Targeting KRAS mutations and their associated pathways remains a therapeutic focus.44
Screening strategies
Target population
Screening focuses on high-risk individuals with a family history or pathogenic germline mutations (e.g. cyclin-dependent kinase inhibitor 2A [CDKN2A], protease serine 1 [PRSS1], breast cancer gene 2 [BRCA2]).45
When to screen
The International Consortium for Pancreatic Cancer Screening (CAPS) provides age-specific recommendations for initiating screening (Supplementary Table 6).45 The age for discontinuation of screening is not clearly stated in any guideline, but similarly to other premalignant conditions, 75–80 years is possibly a reasonable age to stop it, as well as in individuals no longer eligible for pancreatic surgery.45
How to screen
The CAPS guidelines recommend MRI, EUS and glucose testing (HbA1c/fasting glucose). Follow-up intervals depend on lesion size, main pancreatic duct (MPD) dilation and alarming cystic features:
-
Six-month intervals for cysts ≥3 cm, MPD dilation (5–9 mm) or elevated CA19-9.
-
Three-month intervals for solid lesions <5 mm or MPD stricture/dilation ≥5 mm.46
Treatment and management
The standard treatment for PC primarily depends on the tumour extent and its invasion into surrounding structures, such as the superior mesenteric and gastroduodenal arteries.47 PC is classified into four categories: resectable, borderline resectable, unresectable locally advanced and metastatic.
The role of surgery
Surgery is the only definitive treatment for PC and improves outcomes in eligible patients.48 Innovative approaches, such as laparoscopic pancreaticoduodenectomy (LPD) and robotic pancreaticoduodenectomy (RPD), have emerged to enhance survival and reduce postoperative risks. However, their implementation requires skilled surgeons, and their benefits compared with the traditional open approach remain under study. A 2024 retrospective cohort study comparing LPD with open surgery found comparable outcomes, including similar overall survival (OS), blood loss (300 mL each) and postoperative hospital stay (12.0 versus 12.5 days). However, LPD had fewer Clavien–Dindo complications (35.0% versus 66.7%) despite longer operation times (419 versus 325 min).49 Another study on LPD with vein resections reported reduced intraoperative blood loss (200 versus 400 mL) and shorter hospital stay (11 versus 14 days), but longer operation times (390 versus 334 min) compared with the open approach. Both approaches have achieved the same R0 resection rates.50
A meta-analysis of 1,206 patients comparing LPD and open surgery found that LPD reduced blood loss and shortened hospital stay, but longer operation times. Other outcomes, including intensive care unit (ICU) stay, postoperative complications and mortality, showed no significant differences, indicating that LPD offers limited advantages over open surgery.51
RPD has shown advantages over LPD, including reduced blood loss (400 versus 575 mL), lower conversion rates (4.3% versus 29.6%) and shorter hospital stay (11 versus 13 days). However, operation times were similar (approximately 430 min), and both methods had equivalent R0 resection rates.52,53 A 2024 meta-analysis of 9,417 patients concluded that RPD had better outcomes, including lower morbidity (relative risk [RR]: 0.79), shorter hospital stay (mean difference [MD]: –0.72 days) and fewer transfusions (RR: 0.61). LPD and RPD showed similar oncological efficacy, with no significant differences in operation times or R0 resection rates.54
Many studies on LPD and RPD have limitations, such as small sample sizes and retrospective designs. A single-centre study found that RPD had better OS (94.7%, 84.7% and 50.8% at various intervals) compared with LPD (84.1%, 63.6% and 45.5%), but acknowledged the potential bias due to its specialized setting.55
The role of neoadjuvant chemotherapy
Neoadjuvant chemotherapy (NAC) for PC is under active investigation, with studies exploring its efficacy across various disease stages.56,57 Although surgical resection remains the primary curative option, NAC is increasingly utilized in borderline resectable and locally advanced pancreatic cancer (LAPC).
A multicentre phase II trial (A phase I/II clinical trial to verify the safety and efficacy of gemcitabine + nab-paclitaxel + S-1 (GAS) as neoadjuvant chemotherapy for locally advanced pancreatic cancer; Japan Registry of Clinical Trials identifier: jRCTs061180045; University Medical Information Network Clinical Trial Registry number: UMIN000016630) demonstrated that gemcitabine, nab-paclitaxel and S1 (GAS) improved outcomes in borderline resectable PC with arterial contact. The 2- and 5-year OS rates were 68.0% and 44.6%, respectively, with a median of 41 months. Tumour diameters were reduced by ≥10%, and CA19-9 levels were decreased by ≥95%.58 Another trial combining NAC with carbon-ion radiotherapy and surgery showed feasibility but emphasized vascular monitoring, although the trial was terminated because of low enrolment.59 A retrospective study from Russia found that NAC benefited patients with elevated CA19-9 levels (>500 IU/mL). In patients with lower levels, OS was similar between NAC and upfront surgery (28.4 versus 33.7 months).60
A study of 4,041 patients revealed better outcomes with multi-agent NAC (35.8-month OS) compared with single-agent NAC (27.4 months) or upfront surgery (27.1 months).61
Springfield et al. found that NAC increased the 12-month OS from 40% with surgery to 77%, with longer NAC courses achieving a 67% 18-month OS.62 Franklin et al. compared NAC alone with NAC combined with radiotherapy in 1,983 patients. NAC alone resulted in longer median OS (33.2 versus 26.8 months), although high-risk patients benefited more from radiotherapy when adjusted for R1 resection.63 A meta-analysis by Huan et al., including 1,159 patients, found that NAC improved R0 resection rates (RR=1.53) and OS compared with upfront surgery, with no significant difference in surgical complications (RR=0.96).64 Koti et al. analysed trends in NAC use, noting an increase from 4.8% in 2006 to 18.8% in 2017, with NAC improving OS (35.2 versus 28.3 months).65 A 2024 trial by Labori et al. comparing FOLFIRINOX (a chemotherapy every 2 weeks for 4 cycles: oxaliplatin, irinotecan, folinic acid, and fluorouracil [bolus and 46-hour infusion] on days 1 and 15) with upfront surgery showed no survival benefit for NAC (median OS: 25.1 versus 38.5 months).66 Conversely, a phase II trial involving 86 patients found that NAC improved 1-year OS (39% with surgery versus 78–84% with NAC regimens) and disease-free survival (33% versus 59%).67 Cecchini et al. demonstrated the superiority of FOLFIRINOX over gemcitabine, with an OS of 37.2 versus 16.6 months and an 84% completion rate.68
The role of adjuvant chemotherapy
Adjuvant chemotherapy significantly improves survival rates, even in metastatic disease.69,70 Combinations of regimens such as FOLFIRINOX and nab-paclitaxel with gemcitabine (nab-p/Gem) are more effective than gemcitabine monotherapy.70 A 2024 phase II trial reported a 12-month OS rate of 55.3% (95% confidence interval [CI]: 44.2–66.5) for patients receiving nab-p/Gem followed by modified FOLFOX-6 (nab-p/Gem-mFOLFOX), compared with 35.4% (95% CI: 24.9–46.0) for standard nab-p/Gem (p=0.02).71
Another trial assessed adjuvant portal vein infusion chemotherapy (5-fluorouracil and heparin) combined with systemic mitomycin C, cisplatin and gemcitabine administration after surgical resection. The study showed a 10-month OS rate of 44.4% and a 10-year relapse-free survival rate of 38.1%.69 Despite these advancements, chemotherapy resistance remains a major challenge, underscoring the need for targeted therapies.72,73
The role of radiation therapy
Radiotherapy plays a key role in managing advanced PC by improving local control, reducing pain and enhancing quality of life (QoL). Historically, non-ablative five-fraction radiotherapy has been the standard approach. However, a phase II trial of 136 patients with locally advanced or borderline resectable PC demonstrated a 1-year OS rate of 65.0% using ablative five-fraction stereotactic magnetic resonance-guided adaptive radiation therapy, suggesting a potential survival benefit.74
In contrast, a 2024 trial evaluating MRI-guided stereotactic ablative body radiotherapy and CT-guided percutaneous irreversible electroporation following FOLFIRINOX chemotherapy found no improvement in OS or reduction in side effects, indicating no added advantage over standard treatments.75
Another 2024 trial investigated hypofractionated proton beam radiation combined with adjuvant chemotherapy in nine patients after pancreaticoduodenectomy. While no local recurrences were observed, five patients developed distant metastases. The median OS was not reached, but the findings suggest the need for larger phase II trials to assess its safety and efficacy.76
Emerging novel therapeutics
Immunotherapy and cancer vaccines
Immunotherapy for pancreatic ductal adenocarcinoma holds promise despite challenges. Combination therapies, particularly immunotherapy with chemotherapy or chemoradiation, have shown potential. Neoadjuvant immunotherapy has demonstrated encouraging response rates, suggesting that early integration into treatment protocols may improve outcomes.77
Immune checkpoint inhibitors (ICIs) are effective in immunogenic cancers but show limited efficacy in non-immunogenic tumours such as pancreatic ductal adenocarcinoma. Combining ICIs with radiotherapy induces immunogenic cell death, enhances T-cell activation and modulates the TME.78 A study on advanced pancreatic ductal adenocarcinoma treated with programmed cell death protein 1 (PD-1) inhibitors reported a 9.6% hyperprogressive disease rate (10/104) and a poor prognosis (median OS: 3.6 months).79
Many studies have explored ICIs combined with chemotherapy and/or radiotherapy for LAPC (Table 1).30–37 These combinations aim to overcome the modest efficacy of chemotherapy alone by enhancing antitumour responses. In terms of cancer vaccine, Table 2 illustrates many studies that explored this important field.38–42 Figure 2 illustrates emerging therapies for PC.
Table 1: The clinical trials of combination of immune checkpoint inhibitors with other immune agents, chemotherapy ± radiotherapy for locally advanced pancreatic cancer, borderline resectable pancreatic cancer and metastatic pancreatic ductal adenocarcinoma30–37
| Type of trials (immune versus chemotherapy) | Reference | Study design | Country | Patient demographic | Sample size | Immune checkpoint inhibitor | Other agents | Objectives | Results | Conclusion | Limitations |
| Chemotherapy | Chen et al. 202330 | Prospective cohort study | China | Locally advanced pancreatic adenocarcinoma | 96 | Camrelizumab (PD-1 inhibitor) | Nab-paclitaxel, gemcitabine, radiotherapy | Evaluate efficacy and safety of combination treatment versus chemotherapy alone | Combination treatment improved survival rates significantly | Combination therapy was effective and safe for patients with LAPC | Not discussed |
| Immunotherapy | Chen et al. 202331 | Phase II | Denmark | Refractory pancreatic cancer | 26 | Ipilimumab (PD-1 inhibitor), nivolumab (CTLA-4 inhibitor) | Tocilizumab, stereotactic body radiotherapy | Assess efficacy of combined immunotherapy with radiotherapy | No responses observed; 19% had stable disease | Combination did not meet criteria for full accrual | Small sample size, short follow-up |
| Immunotherapy | Lemech et al. 202332 | Phase Ib | Australia | Microsatellite-stable metastatic cancers | 58 | Nivolumab (PD-1 inhibitor) | Pixatimod (TLR9 agonist, a novel immunomodulatory agent) | Determine safety and antitumour activity | No responders in pancreatic cohort; some clinical benefit in colorectal cohort | Pixatimod is well tolerated with nivolumab; further investigation needed | Not specified |
| Targeted therapy | Hernando-Calvo et al. 202433 | Phase II, randomized | Canada | Mismatch repair–proficient cancers | 50 | Durvalumab (PD-L1 inhibitor) | Olaparib (PARP inhibitor), cediranib (VEGFR inhibitor) | Explore combination efficacy | Limited antitumour activity observed | Combinations had limited efficacy; different immune components associated with outcomes | Larger, diverse cohort needed |
| Chemotherapy | Du et al. 202334 | Phase II | China | BRPC/LAPC | 29 | Tislelizumab (PD-1 inhibitor) | Neoadjuvant gemcitabine plus nab-paclitaxel (AG) chemotherapy and concurrent SBRT | Evaluate antitumour activity and safety | High resection rates, 60% ORR | Effective preoperative therapy, promising biomarkers identified | Not discussed |
| Chemotherapy | Enzler et al. 202435 | Phase II, randomized | USA | Advanced pancreatic adenocarcinoma | 36 | Nivolumab (PD-1 inhibitor) | CBP501 (calmodulin-binding peptide), cisplatin | Establish efficacy of combinations | Partial responses in one arm; no responses in others | Some signs of efficacy; well tolerated | Sample size, short duration |
| Chemotherapy | Zhou et al. 202436 | Retrospective study | China | Locally advanced pancreatic adenocarcinoma | 64 | Sintilimab (PD-1 inhibitor) | S-1 and gemcitabine chemoradiotherapy | Assess feasibility and efficacy | Improved survival rates in treatment group | Effective and safe, warrants further investigation | Retrospective design |
| Targeted therapy | Ko et al. 202337 | Phase Ib/II | Multiple international sites | Advanced pancreatic and gastric cancers | 79 | Atezolizumab (PD-L1 inhibitor) | PEGPH20 | Evaluate efficacy and safety | Limited activity in pancreatic cancer; none in gastric cancer | Limited clinical activity, safety profile consistent | Larger cohort needed for robust conclusions |
ADP = adenosine diphosphate; AG = nab-paclitaxel plus gemcitabine; BRPC = borderline resectable pancreatic cancer; CTLA-4 = cytotoxic T-lymphocyte-associated protein 4; LAPC = locally advanced pancreatic cancer; ORR = objective response rate; PARP = poly (ADP-ribose) polymerase; PD-1 = programmed cell death protein 1; PD-L1 = programmed death-ligand 1; PEG = polyethylene glycol; PEGPH20 = PEGylated recombinant human hyaluronidase; SBRT = stereotactic body radiotherapy; TLR9 = toll-like receptor 9; VEGFR = vascular endothelial growth factor receptor.
Table 2: Oncology vaccine38–42
| Reference | Study type | Country | Patient demographic | Sample size | Cancer vaccine | Mechanism of action | Outcomes | Conclusion | Limitations |
| Meng et al. 202338 | Research article | China | Murine models | Not specified | Whole TCV | Photothermal nanoparticle-loaded tumour cells induce heat shock proteins as adjuvants. Near-infrared laser irradiation promotes immune cell recruitment and activation | Increased antitumour immune responses, effective across different murine models | TCV platform shows promise for personalized immunotherapy | Specifics on long-term immune memory not discussed |
| Pant et al. 202439 | Phase I clinical trial | International | Patients with pancreatic and colorectal cancer | 25 | ELI-002 2P | Amphiphile modification enhances lymph node delivery and immune response | Positive tumour biomarker response in 84% of patients, median RFS of 16.33 months | Amphiphile vaccine shows promising T-cell responses and tumour biomarker reduction | Small sample size limits broader conclusions |
| Raman et al. 202340 | Original research | USA | Mice with pancreatic tumours | Not specified | ID Salmonella delivering ovalbumin | Salmonella induces cell lysis to release proteins directly into the cytoplasm, facilitating antigen cross-presentation | Elimination of tumours in treated mice, increased survival | Effective in refocusing immune responses and eliminating tumours | Translation to human efficacy not discussed |
| Heumann et al. 202341 | Clinical trial | USA | Patients with resectable pancreatic adenocarcinoma | 40 | GVAX + nivolumab and urelumab (anti-CD137 agonist) | GVAX induces T-cell responses, combined with ICIs to enhance immune activity | Improved T-cell activation, potential increase in survival rates | Shows potential for combination vaccine and ICI therapy in pancreatic cancer | Small cohort, conclusions not definitive |
| Van’t Land et al. 202442 | Clinical trial | Netherlands | Patients with resected pancreatic cancer | 38 | Dendritic cell vaccine pulsed with tumour cell lysate | Dendritic cells activate T cells against pancreatic cancer antigens | 64% of patients did not develop recurrence after 2 years | Promising results for preventing recurrence in pancreatic cancer post-surgery | Limited to single-centre and small sample size |
CD137 = cluster of differentiation 137; GVAX = granulocyte-macrophage colony-stimulating factor–gene-modified tumour vaccine; ICI = immune checkpoint inhibitor; ID = intraduodenal; RFS = relapse-free survival; TCV = tumour cell vaccine.
Figure 2: Emerging therapies in cancer treatment
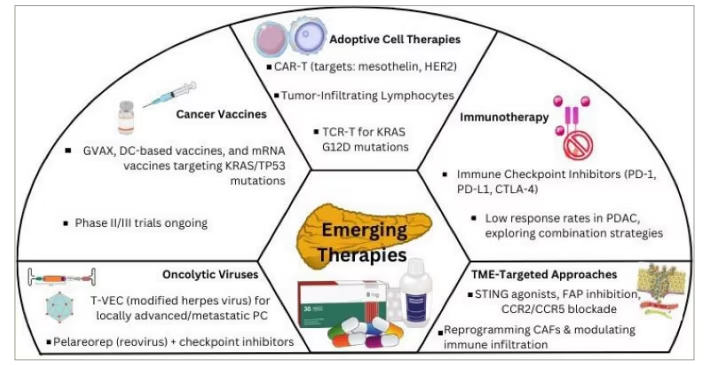
Figure created with Canva.com.
CAF = cancer-associated fibroblast; CAR-T = chimeric antigen receptor T cell; CCR = chemokine (C-C motif) receptor; CTLA = cytotoxic T-lymphocyte-associated antigen; DC = dendritic cell; FAP = fibroblast activation protein; GVAX = GM-CSF–secreting vaccine; HER2 = human epidermal growth factor receptor 2; KRAS G12D = KRAS Gly12Asp mutation; mRNA = messenger RNA; PC = pancreatic cancer; PD = progressive disease; PD-L = programmed death ligand; PDAC = pancreatic ductal adenocarcinoma; STING = stimulator of interferon genes; TCR-T = T-cell receptor–engineered T cell; TP53 = tumour protein 53; T-VEC = talimogene laherparepvec.
Additionally, ELI-002 2P, a KRAS-mutated peptides vaccine, is given to high-risk post-operative patients, attacking KRAS-mutated cells by eliciting a T-cell response in patients with immunotherapy-recalcitrant KRAS-mutated tumours. In a phase I trial, 84% of patients developed KRAS–specific T-cell responses.80 Also, a personalized messenger ribonucleic acid (mRNA)-based vaccine, autogene cevumeran, has been found to delay the recurrence by eliciting a strong post-operative T-cell response.81 Both of these vaccines are currently being explored in randomized phase II trials.
Emerging immune targets
-
Targeting chemokines: C-C chemokine receptor 2/C-C chemokine receptor 5 (CCR2/CCR5) receptors regulate immune cell migration via C-X-C motif chemokine ligand (CXCL) ligands. A phase I/II trial in LAPC evaluated a chemokine receptor inhibitor combined with immunotherapy after chemotherapy and radiation.82 Phase I enrolled patients with a median age of 67, of whom 70% were male. Nearly 70% of the patients underwent immunotherapy, with no reported dose-limiting toxicities. The only grade ≥3 adverse event was rash (8%), and the recommended phase II dose was established. This trial is currently on-going.83 Trials targeting CXCL2 are also on-going.84
-
Innate immunity: The stimulator of interferon genes (STING) pathway plays a key role in innate immunity by reducing tumour burden and inducing inflammation. Lipid nanoparticle-encapsulated STING agonists cyclic GMP-AMP–loaded lipid nanoparticles (cGAMP-LNPs) enhance efficacy and mitigate toxicity in preclinical models.85 Combining STING agonists with ICIs is promising, as STING activation upregulates immune checkpoint ligands.86 A phase I trial tested granulocyte-macrophage colony-stimulating factor–gene-modified tumour vaccine (GVAX) and pembrolizumab, which showed enhanced CD8+ T-cell activation and a 78% pathological response rate.87 Interleukin-18 receptor (IL-18R) signalling is another potential target, with blockade strategies showing enhanced efficacy when combined with PD-1 inhibitors.88
-
Adoptive cell therapy (ACT): ACT uses autologous immune cells, such as T cells, to target pancreatic ductal adenocarcinoma cells. Despite low neoantigen expression, antigenic diversity, particularly in KRAS mutations, poses a challenge.89
-
T-cell receptor (TCR) engineering: TCRs conjugated to cluster of differentiation 3 (CD3) initiate T-cell activation contingent on human leukocyte antigen (HLA) restriction.90,91 A phase I trial investigated KRAS G12D-targeting TCRs in advanced or metastatic pancreatic ductal adenocarcinoma, whereas another evaluated mesothelin-specific TCR-T cells with chemotherapy for metastatic pancreatic ductal adenocarcinoma, aiming for an overall response rate of >20%.92,93
-
Chimeric antigen receptor T-cell (CAR-T) therapy: CAR-T therapy uses genetically engineered T cells expressing chimeric receptors that target tumour-associated antigens. Challenges include antigen diversity and immunosuppressive microenvironments. A novel approach uses mesothelin-targeting CAR-T cells that secrete T-cell-engaging molecules (TEAMs) to modify the tumour stroma and enhance T-cell activation.94 Studies have demonstrated the potent antitumour activity of interleukin-7/C-C motif chemokine ligand 19 (IL-7/CCL19)-secreting CAR-T cells in human epidermal growth factor receptor 2 (HER2)-positive PC models.95 A novel immunotherapy uses mesothelin-targeting CAR-T cells secreting TEAM to inhibit cancer-associated fibroblasts (CAFs) via fibroblast activation protein (FAP), improve the TME and enhance antitumour efficacy in pancreatic ductal adenocarcinoma. Mesothelin-targeted fibroblast activation protein (MesoFAP) CAR-TEAM therapy effectively modified the tumour stroma, boosting T-cell activation and cytotoxicity.96
-
Tumour-infiltrating lymphocytes (TILs) and oncolytic viruses therapy: TIL therapy involves surgical tumour resection, ex vivo evolution and reinfusion of autologous TILs to activate antitumour immunity.97
Building on this concept, oncolytic virus-based approaches have been explored to enhance immune responses. A phase II trial combining pelareorep, an oncolytic reovirus, with pembrolizumab without chemotherapy to preserve viral-mediated antitumour effects achieved a 42% clinical benefit rate among 12 patients with advanced pancreatic ductal adenocarcinoma, accompanied by immunological changes including decreased CD4+ regulatory T cell (Treg) levels in responders.98 Another trial investigated talimogene laherparepvec, a modified herpes virus, in patients with locally advanced or metastatic PC who had failed prior to chemotherapy.99 Preclinical studies of the Oncotech approach, which combines engineered oncolytic adenoviruses with programmed death-ligand 1 (PD-L1)-targeted T cells, demonstrated enhanced tumour infiltration and downregulation of PD-L1 expression, highlighting the promise of combining oncolytic virotherapy with cell therapy for cancer treatment.100 Despite these advances, response rates in PC remain generally poor.98–100
Quality of life and tumour burden
Maintaining the QoL is vital for patients who face significant physical, emotional and social challenges. Various tools assess QoL, such as the EORTC QLQ-C30 and disease-specific instruments such as FACT-PA and FACT-HEP. However, differences in instrument selection, assessment frequency, patient compliance and follow-up duration limit the consistency and applicability in clinical trials.101
Pain and malnutrition
Pain is a common and debilitating symptom, particularly in the advanced stages.102 It may arise from tumour invasion of nerve fibres or ducts, or from treatment-related side effects.103
Management options include:
-
Pharmacological: Nonsteroidal anti-inflammatory drugs (NSAIDs), opioids (e.g. morphine), corticosteroids and neuropathic agents (e.g. gabapentin, pregabalin).102
-
Non-pharmacological: Coeliac plexus nerve blocks, neurolysis and radiation therapy.104
The phase II PAINPANC trial demonstrated significant pain reduction and QoL improvement with short-course palliative radiation therapy, with only mild toxicity.105 Complementary therapies, such as self-acupressure, may offer additional relief.106 Early pain management is essential for improving physical and mental wellbeing.103
More than 60% of patients with PC experience weight loss and malnutrition at diagnosis.107 Causes include metabolic changes, reduced appetite, taste dysfunction, early satiety, nausea and pancreatic exocrine insufficiency (PEI) (affecting 80% of post-surgery cases and 92% of advanced cases).108 Cachexia (80% prevalence) and sarcopenia (50%) further worsen outcomes, increasing complications, treatment intolerance and mortality.109,110 Interventions to improve absorption and outcomes include oral nutritional supplements, enteral feeding, parenteral nutrition and pancreatic enzyme replacement therapy.111 Preoperative immunonutrition enriched with arginine and omega-3 fatty acids enhances recovery, reduces infection rates and boosts immune function.112
Physical activity and prehabilitation
Physical activity improves QoL by reducing side effects, fatigue and pain while enhancing sleep, mood and functional capacity.113,114 It also mitigates cachexia and sarcopenia.115 Personalized programmes, tailored by type, intensity and feasibility, are essential for safe and effective integration into patient care.114
Prehabilitation, focusing on nutritional, physical and psychological optimization before surgery, shows promise in improving outcomes. A systematic review of 12 studies (1,497 patients) found that prehabilitation improved functional capacity (6 min walk test) and reduced pulmonary complications (2.4% versus 6.7%; RR: 0.36) but had no significant effect on overall complications, length of stay or mortality.116 Standardized prehabilitation guidelines integrated with Enhanced Recovery After Surgery protocols are needed to enhance its effectiveness.117
Psychological and caregiver burden
PC diagnosis often leads to anxiety, depression and cognitive dysfunction owing to poor prognosis and severe symptoms. A biological link between PC and depression has been suggested.118 Early interventions, including pharmacotherapy, psychotherapy, meditation and emotional support, are crucial for mental health.119,120
Mental health issues can disrupt daily activities and social interactions, often leading to isolation.121 Strong social support from family, friends and healthcare providers is vital. Caregivers face significant challenges, including symptom management, decision-making and financial burden, often experiencing unmet needs in education and healthcare communication.122–124 Dyadic positive coping strategies and referrals to palliative care, which address both patient and caregiver needs, can alleviate these burdens.125
Economic burden
PC imposes a substantial economic burden owing to its late detection, short survival times and aggressive treatments. In 2016, PC treatment costs in the USA totalled $2.5 billion, with projections exceeding $4 billion by 2040.126 In Europe, costs were €124 million in 2016, which are expected to reach €210 million by 2030.127 Indirect costs from lost productivity surpass direct medical expenses, exacerbating financial toxicity (FT), which affects treatment adherence and QoL.128,129 Policies addressing FT, early detection programmes and investments in cost-effective treatments are essential for mitigating economic strain.129
Multidisciplinary teams and precision in medicine
Given the complexity of PC, multidisciplinary teams (MDTs) involving specialists from various fields are critical for optimizing treatment and improving outcomes. Recent studies have highlighted the significant role of MDTs in PC management. Francisse et al. showed that MDT discussions led to diagnostic changes in 92 of 522 patients and treatment plan alterations in 377. Patients with an initial diagnosis of solid tumours (64.9%) or cystic lesions (35.4%) benefited from MDT assessments, with most referrals (66.9%) focusing on therapeutic management.130
Similarly, Quero et al. found that MDTs improve surgical eligibility and diagnostic accuracy. Of 487 patients, 89 experienced changes in treatment, 31 underwent diagnostic revisions and 45 underwent reassessment of resectability.131 In Denmark, Pedersen et al. reported that MDTs detected premalignant lesions in approximately 8% of 455 patients, preventing missed diagnoses.132 However, access to MDT care can be limited. Patients receiving MDT care had access to more treatment options and better survival outcomes (median survival: 5.9 versus 4.5 months for non-MDT patients).133
Artificial intelligence in pancreatic cancer
The integration of artificial intelligence (AI) into clinical practice is transforming PC management, with advancements in diagnosis, biomarker detection, treatment and prognosis (Figure 3).134
Figure 3: Artificial intelligence applications in pancreatic cancer
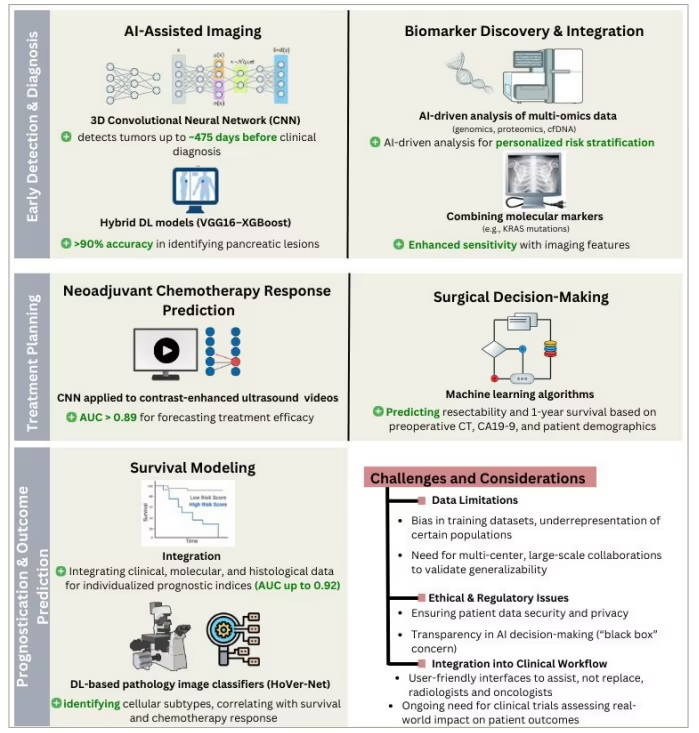
Figure created with Canva.com.
AI = artificial intelligence; AUC = area under curve; CA19-9 = carbohydrate antigen 19-9; CFDNA = circulating free DNA; CT = computed tomography; CNN = convolutional neural network; DL = deep learning; KRAS = kirsten rat sarcoma virus.
The early diagnosis of PC is challenging because of nonspecific symptoms and the absence of early-stage indicators. Tumour size and CA19-9 levels are often critical in the later stages. AI models can enhance diagnostic accuracy by capturing more details while saving time and effort. Korfiatis et al. developed a 3D convolutional neural network (CNN) trained on non-neoplastic PC CT scans, achieving a mean accuracy of 92%, sensitivity of 88% and specificity of 95%. Notably, it detected occult preinvasive PC up to a median of 475 days before clinical diagnosis, showing promise for T1-stage PC screening.135 Similarly, a hybrid deep learning (DL) model (VGG16–XGBoost) classified pancreatic ductal adenocarcinoma CT images based on tumour, node, metastasis (TNM) staging and achieved 97% accuracy.136
Another model combining CNN and YOLO (You Only Look Once) classifies PC grades using pathological images and CT scans. Although it requires further improvement with advanced DL models and larger datasets, it serves as a valuable second-opinion tool for pathologists.137 A DL-based model for predicting lymph node metastasis from multiphase CT images achieved 74.4% accuracy, highlighting the need for future advancements in this area.138
A particularly promising tool is PC detection with AI (PANDA), which detects and classifies pancreatic lesions using non-contrast CT with a sensitivity of 92.9% and specificity of 99.9%. PANDA has already demonstrated its potential for the correct detection of other cancers, specifically cancer types (oesophagus, liver, stomach), for which no guideline recommends screening tests available for average-risk groups.139 PANDA could serve as a new tool for large-scale PC screening, and we hope that it will help in changing the current cancer-detection paradigm from late-stage screening to one in which cancer can be detected before symptoms appear.139 Although PANDA shows promise, it is still under investigation, and it is now trained on a continual learning approach using multi-centre data. However, it includes limited data from outside the East Asian population and hospitals. Accordingly, PANDA needs more validation in diverse populations and external real-world centres.139
AI has also improved the treatment strategies. Two CNN models applied to contrast-enhanced ultrasound videos predicted NAC efficacy in PC, with AUCs of 0.892 and 0.908, correctly classifying over 40% of the videos. These findings provide a foundation for further refinement.140 The HoVer-Net DL model predicted disease-specific survival in patients with pancreatic ductal adenocarcinoma undergoing adjuvant gemcitabine treatment. Using histological features, it categorizes nuclei into five classes: neoplastic, connective, non-neoplastic/epithelial, necrotic and inflammatory, offering potential time and cost savings.141
Another model predicted 1-year survival in patients with pancreatic ductal adenocarcinoma undergoing pancreaticoduodenectomy using preoperative features (e.g. age, sex, CA19-9 and imaging). Tree regression achieved an AUC of 0.92, whereas logistic regression reached 0.74, aiding personalized treatment decisions.142 Additionally, a model using clinical and multi-omic molecular data, including RNA sequencing of 648 genes, predicted disease survival and identified biomarkers for future therapies.143
Research gaps and future directions
Early detection of PC remains challenging owing to its asymptomatic nature and the absence of specific biomarkers. Effective screening, particularly for high-risk populations, is crucial to improve outcomes; however, balancing sensitivity and specificity is difficult and may lead to false positives, imposing psychological and economic burdens. The emotional impact of ambiguous or positive results further complicates screening in these groups.46
NAC shows promise for resectable and borderline resectable cases, but issues such as potential metastasis during NAC and surgical delays due to side effects persist. Several trials have been halted owing to poor accrual, underscoring the need for further studies to optimize NAC protocols.144 Similarly, although radiotherapy may aid local control, its side effects on pancreatic tissues require further investigation to validate its overall benefit.145
Moreover, additional variables such as genetic profiles, biomarkers and patient performance status are not yet fully integrated into staging systems, highlighting the need for more personalized approaches.146–148 Finally, AI applications face challenges, including limited datasets, bias in sex and race representation, and concerns about data safety and transparency.149,150
MDT adoption faces barriers, such as lack of awareness, decision-making complexity and cost. Solutions such as remote consultations and AI integration may enhance MDT implementation and accessibility.151
Conclusion
PC continues to be a serious clinical challenge because of its aggressive biology, late diagnosis and limited effective treatment options. This article highlights the complex molecular landscape of PC, underscored by key genetic mutations and intricate interactions within the TME that drive disease progression and resistance to therapy. Although conventional treatment modalities, such as surgery, chemotherapy and radiotherapy, remain central to management, emerging approaches, including neoadjuvant therapies, immunotherapy and AI-driven diagnostic tools, offer promising avenues for improving patient outcomes. Nonetheless, there are considerable gaps, especially in early detection, optimal integration of new interventions and personalization of treatment plans. Future research should address these uncertainties through well-structured clinical trials and collaborative multidisciplinary efforts.